CLINICAL PRESENTATION
Patient
Male, 60s – presenting to the Emergency Department
Chief Complaint
- Right upper quadrant (RUQ) pain
- Leukocytosis on labs
Initial Workup
- RUQ ultrasound obtained
- Followed by CT abdomen & pelvis
Positive Findings
- Sonographic Murphy sign positive on sonography
- Severe tenderness with probe pressure over GB
Transverse GB — Color Doppler Ultrasound
⚠️ RUQ pain + leukocytosis + positive Murphy sign → high suspicion for acute cholecystitis requiring urgent imaging
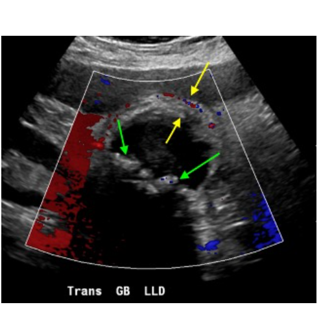
🟢 Green arrows
Echogenic foci within the GB lumen casting posterior acoustic shadows – consistent with cholelithiasis (gallstones).
🟡 Yellow arrows
Gallbladder wall markedly thickened and edematous with associated wall hyperemia on color Doppler – a hallmark of acute inflammation.
➕ Additional
Pericholecystic fluid noted. Focal wall discontinuity with complex fluid collection between the GB and liver – raising concern for perforation.
CT ABDOMEN & PELVIS — Confirmatory Imaging
CT Findings
- Pericholecystic fat stranding — surrounding inflammatory response
- Markedly thickened GB wall — confirms acute cholecystitis
- Complex fluid collection in the subhepatic space between the liver and GB
- Focal gallbladder wall discontinuity — evidence of the perforation site
Imaging Interpretation
CT confirms a markedly thickened GB wall with pericholecystic free fluid and fat stranding (green arrows). A focal gap in the GB wall, along with a complex subhepatic fluid collection between the liver and gallbladder, confirms perforation (yellow arrows).
Acute Cholecystitis — Type 2 Gallbladder Perforation with Subhepatic Abscess
Incidence
Perforation complicates fewer than 5% of acute cholecystitis cases, yet significantly raises morbidity and mortality risk.
Underlying Mechanism
Gallstone obstruction of the cystic duct → bile retention → rising intraluminal pressure → ischemia and necrosis of the GB wall → perforation.
At-Risk Population
More prevalent in elderly patients and those with underlying chronic medical conditions; commonly presents with RUQ pain.
Preferred Perforation Site
The GB fundus is most susceptible due to its terminal blood supply and consequent vulnerability to ischemia. Trauma may also precipitate perforation.
Onset of perforation may occur anywhere from 2 days to several weeks following the initial episode of acute cholecystitis.
Type 1 — Acute / Free Perforation
Sudden complete rupture of the gallbladder wall resulting in bile spillage and generalized peritonitis — the most clinically severe form.
Type 2 — Subacute / Localized (Most Common)
Contained perforation forming a pericholecystic abscess or phlegmon. This is what our patient demonstrated.
Type 3 — Chronic / Fistula to Bowel
Gradual erosion of the GB wall leading to a cholecystoenteric fistula — may precipitate gallstone ileus.
Type 4 — Biliary Tree Perforation
Fistulous connection between the gallbladder and the biliary ductal system (cholecystobiliary fistula).
Potential Complications
- Intraperitoneal free air from GB rupture
- Bile leak into the peritoneal cavity
- Hepatic abscess — via direct spread or hematogenous seeding
- Small bowel obstruction (gallstone ileus)
- Sepsis and multi-organ failure if untreated
Treatment Approach
Step 1 — Stabilization
IV antibiotics, IV fluids, pain management, NPO
Step 2 — Percutaneous Cholecystostomy
Tube drainage to decompress the GB and control infection prior to surgery — especially in high-risk or frail patients
Step 3 — Abscess Drainage
CT- or US-guided percutaneous drainage of pericholecystic or subhepatic collection
Step 4 — Definitive Surgery
Cholecystectomy (laparoscopic or open) once inflammation subsides; fistula repair if required
01. Gallbladder perforation, though uncommon, carries a significant risk of morbidity and mortality — early recognition is critical to prevent sepsis and multi-organ failure.
02. A positive sonic Murphy sign on ultrasound is a reliable bedside indicator of acute cholecystitis and should prompt immediate further workup.
03. Ultrasound remains the primary imaging tool for suspected cholecystitis; CT is invaluable for identifying complications such as wall discontinuity and abscess formation.
04. Type 2 perforation (subacute, localized abscess) is the most common subtype — and CT often reveals the pericholecystic collection missed on ultrasound alone.
05. Percutaneous cholecystostomy drainage before cholecystectomy is a viable bridge strategy in elderly or surgically high-risk patients.