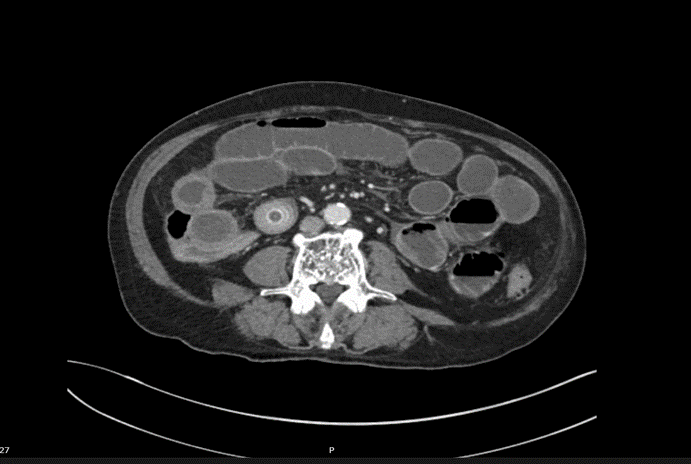
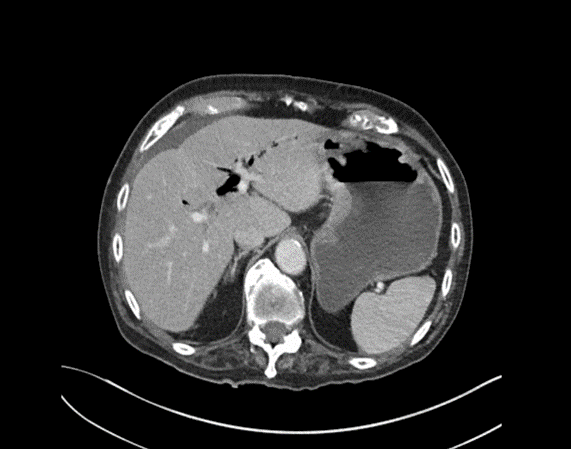
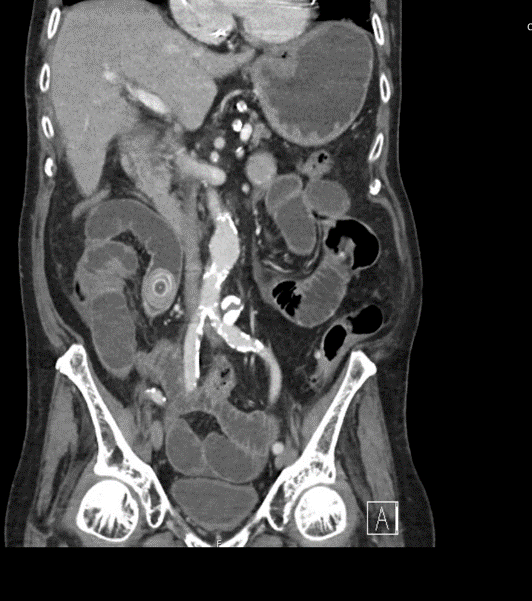
A 92-year-old man presented to emergency with abdominal pain, vomiting and fever. He had been experiencing 24 hours of abdominal pain which had become significantly worse in the last 3 hours. He has generalized abdominal tenderness and distention. Lactate is 2.5 and he has a mild AKI.
Fig.3
Fig.2
Fig.1
EXPLANATION -There are multiple dilated loops of small bowel secondary to small bowel obstruction. There is mild mural thickening in the right lower quadrant, suggestive of early ischemia. An abrupt transition is seen in the terminal ileum due to a 30 mm gallstone – a gallstone ileus.
Pneumobilia is present, this is secondary to a cholecystoduodenal fistula.
Fig.3
Fig.2
Fig.1
Gallstone ileus is an uncommon but potentially serious cause of small bowel obstruction.
It occurs when a gallstone enters the small bowel via a biliary-enteric fistula, causing a mechanical bowel obstruction.
The site of obstruction is the terminal ileum in 50-70% cases (as in this case), 90% of stones over 2cm in diameter cause obstruction. There may be colicky, often periumbilical, abdominal pain, distension, constipation, nausea and vomiting.
Current surgical options are simple enterolithotomy (as in this case); enterolithotomy, cholecystectomy and fistula closure (one-stage procedure) or enterolithotomy with cholecystectomy performed later as a two-stage procedure.
This patient went for urgent laparotomy. A 3cm gallstone was found in the distal ileum. The gallstone was able to be moved proximally, and an enterotomy was performed for removal of the gallstone via the ileum.
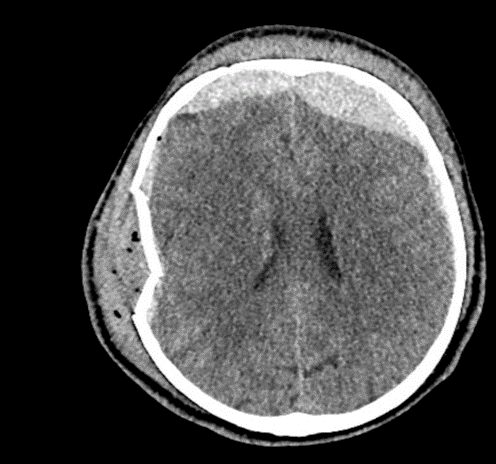
CASE 2 -A 54-year-old man walks into emergency 3 hours after a 150kg plank of wood fell on his head. He has obvious external signs of head injury and a cracking headache, however, neurologically he is intact. A CT head scan is performed
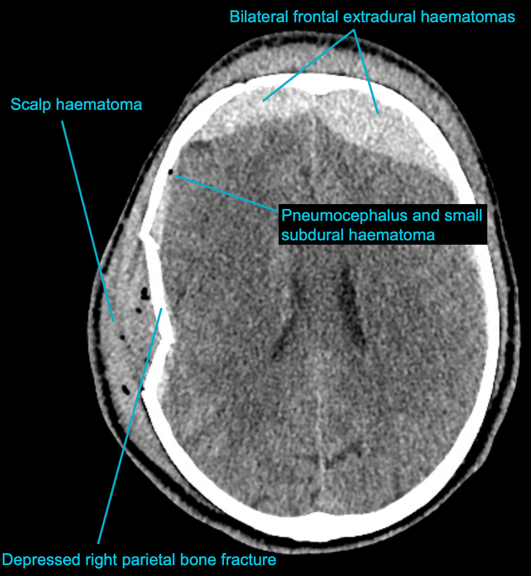
EXPLANATION –There is a depressed right parietal bone fracture with underlying pneumocephalus (indicates an open skull fracture) and a small subdural hematoma.
Overlying this there is a scalp hematoma.
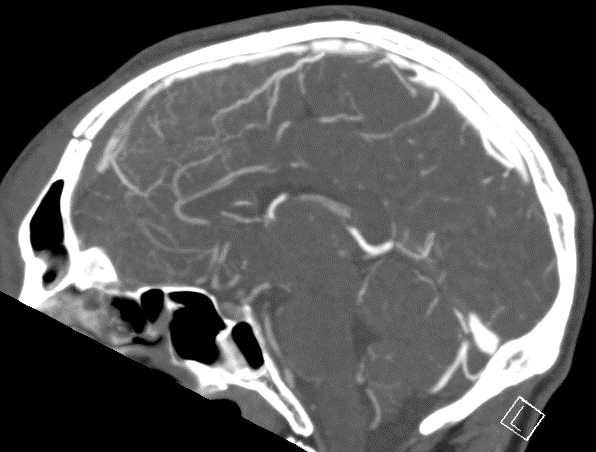
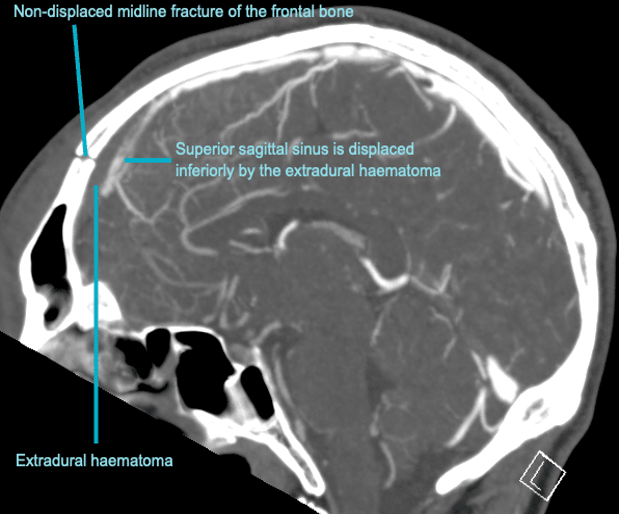
There is also a non-displaced fracture in the frontal bone. This fracture crosses the midline and probably has injured the anterior aspect of the superior sagittal sinus.
Tears of the dural venous sinuses may cause an extradural hematoma (EDH), as in this case. The hematoma is seen external to the compressed superior sagittal sinus.
Fig.1
Fig.2
Extradural bleeds (EDH) are located between the outer layer of dura and endosteal layer of skull. Like in this case, they are usually associated with calvarial fractures.
They typically demonstrate biconvex or lentiform shape and are limited by sutures as periosteum is attached at the sutures limiting spread of the bleed.
The source of bleed is arterial in origin, from a middle meningeal artery as opposed to venous in subdural bleeds.
Up to 10% of EDH are due to venous bleeding, follow the laceration of a dural venous sinus, as we see in this case.
There is often displacement of the sinus away from the underlying bone. There are three locations characteristic of venous EDH; the vertex, anterior middle cranial fossa and the occipital posterior fossa.
Hypodense areas within a bleed likely represent unclotted blood suggesting active bleeding.
As these bleeds are venous, there is not the same urgency for decompression in theatre. In fact, this patient was managed conservatively as operative intervention poses a risk of further damage to the venous sinuses.
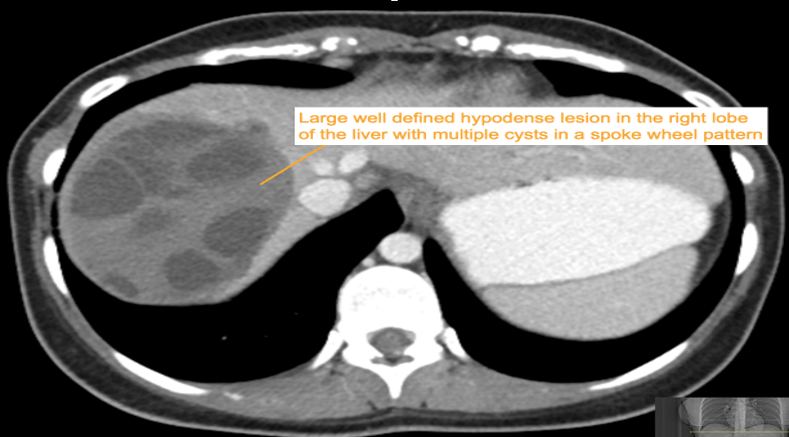
CASE 3 – A 23-year-old woman presents with 3 weeks of right upper quadrant (RUQ) pain associated with early satiety. The patient has no significant past medical history. She was born in Iraq and migrated to Australia from Syria 2 years prior to presentation. Preliminary blood results demonstrate moderate liver function test (LFT) derangement.
Fig. 1
Fig. 2
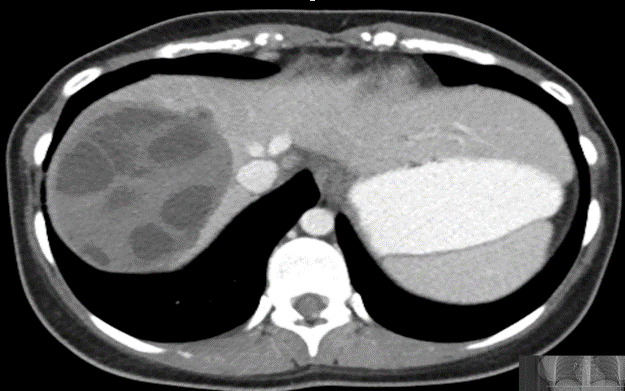
EXPLANATION -The case demonstrates classical appearance of a hepatic hydatid cyst. There is a well-defined rounded lesion in right lobe of liver with multiple small daughter cysts within. The fluid in the cysts can be of variable density depending on the proteinaceous contents (more protein = more dense). The thick internal septae can give a “spoke wheel” appearance as in this case. Curvilinear calcifications represents the inactive stage of the disease.
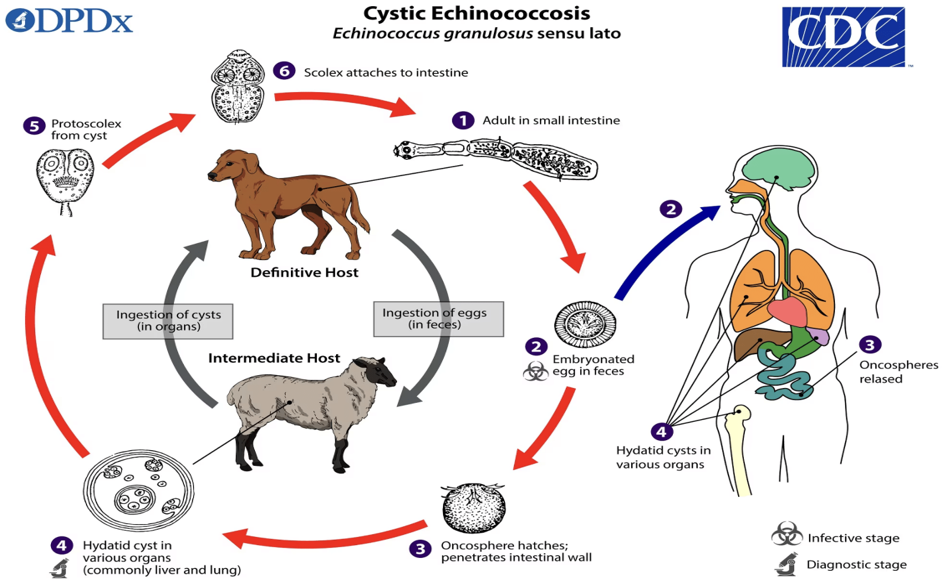
Hydatid diseases a parasitic zoonosis, caused by the larval stages of the Echinococcus granulosus .
E. granulosusis found worldwide, however the highest rates of infection are seen in the Mediterranean and Middle Eastern regions, North Africa and South America.
Hydatid cyst can occur anywhere in the body, the most commonly affected organ is the liver (76% of cases), followed by lung (15%) and spleen (5%).
Classically there is a large ‘parent cyst’ which contains numerus peripheral ‘daughter cysts’.
Humans are infected by eating the eggs of the tapeworm E. granulosus, by either eating contaminated food or through contact with dogs.
The ingested embryos invade the intestinal mucosal wall, enter the portal circulation and develop cysts in the liver.
Treatment options ; Surgical excision, PAIR (Puncture, Aspiration, Injection of protoscolicidal agent and Re-aspiration), Anti-helminthic agent (e.g. albendazole, mebendazole), Observation only – for inactive and silent cysts
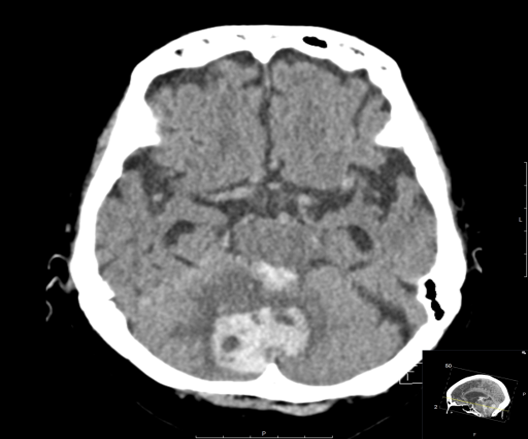
CASE 4 –An 82-year-old female of Asian descent from a nursing home presents with hypertension, nausea and vomiting. Vitals are BP 180/105, HR 65, GCS 8, which soon dropped to 6. Patient is K/C/O atrial fibrillation and is on warfarin. soon after arrival, warfarin was reversed due to suspicion of intracranial hemorrhage and the patient was sent for urgent CT scan.
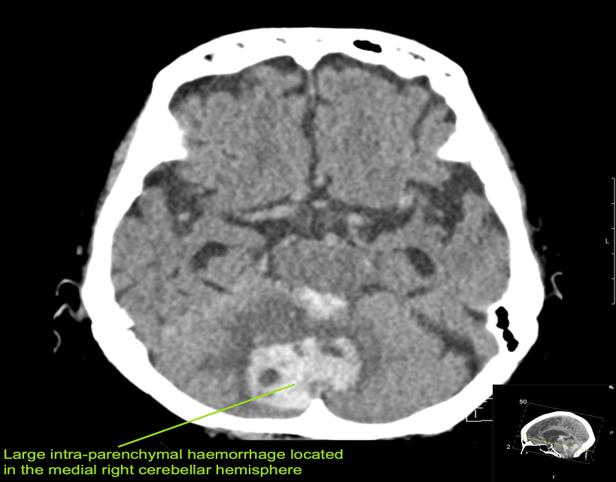
EXPLANATION –There is a large intra-parenchymal hemorrhage located in the medial right cerebellar hemisphere extending into the cerebellar vermis. There is intraventricular extension into the fourth ventricle and aqueduct with mild obstructive hydrocephalus (mild dilatation of the lateral ventricles).
Cerebellar hemorrhage comprise approximately 10% of all intracerebral haemorrhages (ICH).
Typical clinical symptoms are vertigo, ataxia, headache and vomiting. If they progress in size reduced consciousness will follow.
Cerebellar hemorrhage may be related to hypertension, trauma, coagulopathy, hemorrhagic transformation of ischemic strokes, as well as underlying vascular abnormalities such as AVMs.
Incidence increases with age and is most prevalent in Asian populations, as in our patient.
Cerebellar bleeds are a neurosurgical emergency with urgent referral required due to the risk of mass effect and brain stem compression, cerebellar herniation and resultant hydrocephalus.
This bleed was deemed nonsurvivable and the patient was managed on a palliative pathway. Amazingly, the next day she made a neurological recovery, she was obeying commands and ultimately returned to her nursing home.
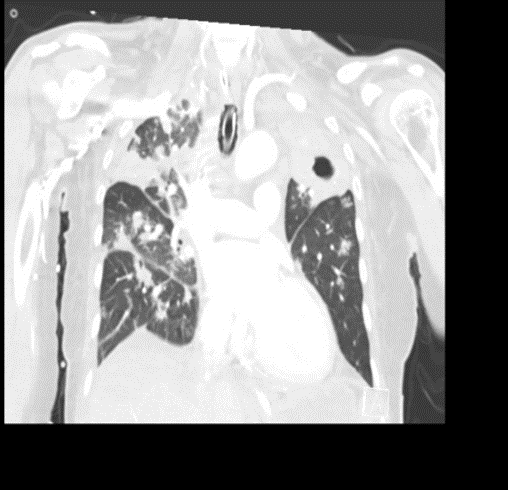
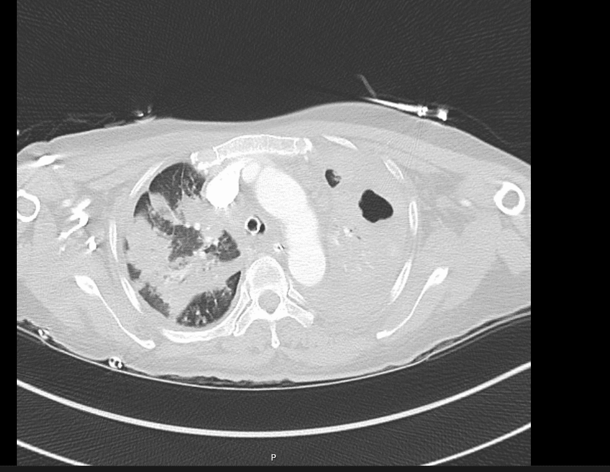
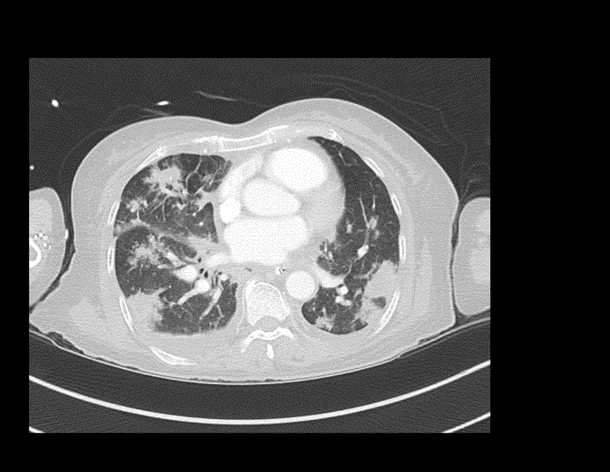
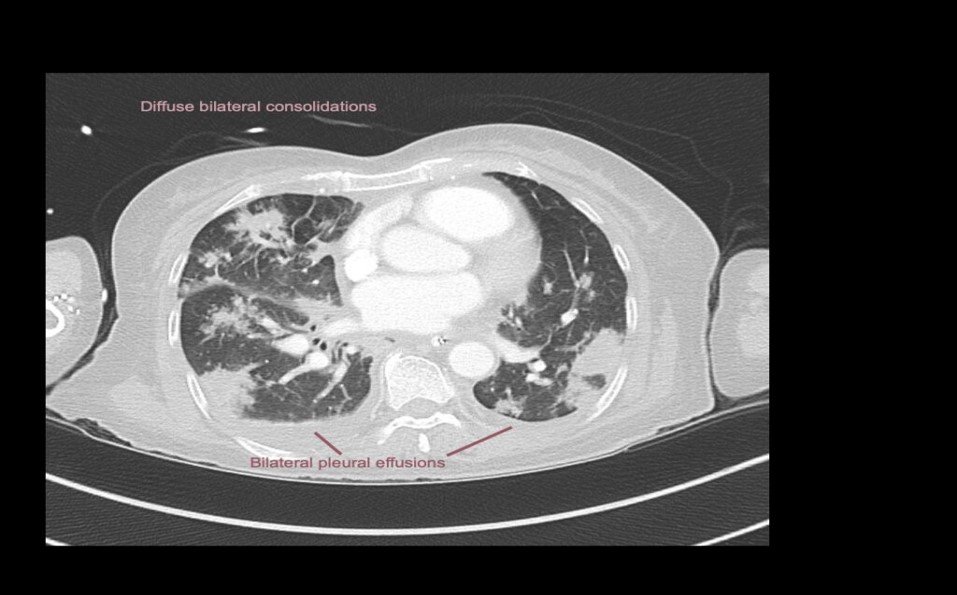
CASE 5 –A 57-year-old woman presented to the emergency department with fevers, cough and night sweats and recent weight loss. She arrived in Australia from Philippines 5 days previously. In the ED she had significant respiratory distress requiring high flow oxygen and subsequent intubation and ventilation as her respiratory failure progressed.
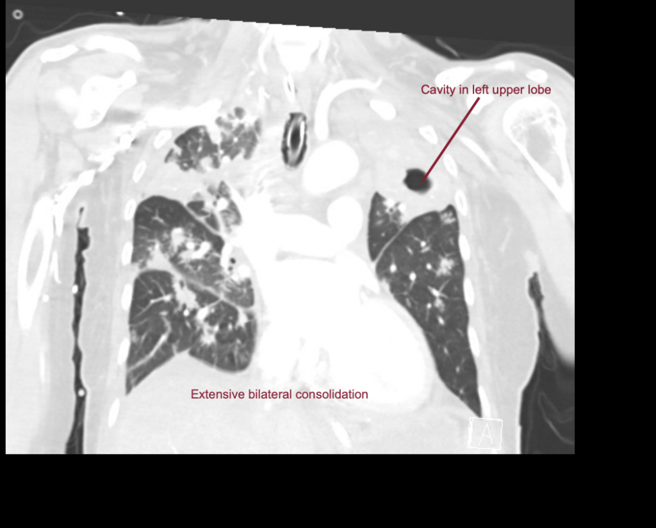
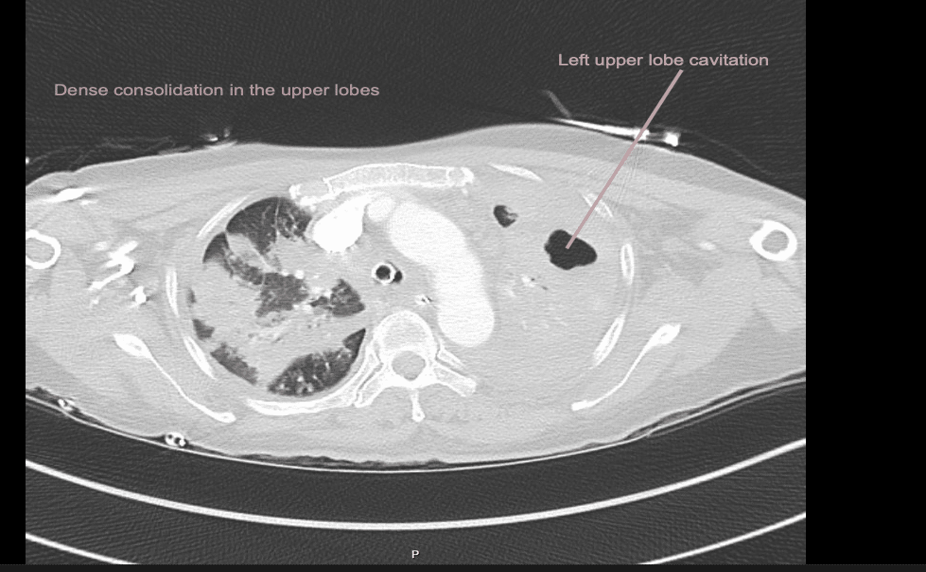
EXPLANATION -There is diffuse bilateral consolidation more prominent in the upper lobes.
There is left upper lobe cavitation. Bilaterally there are pleural effusions.
TB is caused by Mycobacterium tuberculosis, and very rarely by Mycobacterium bovis.
Tuberculosis can manifest in any organ, with the more common locations being kidneys, spine (Pott’s disease) and the brain.
Transmission occurs via inhalation of infectious aerosols.
In countries like Australia(as in our case), it is a notifiable disease.
She had +ve AFB in her sputum which fortunately was treatment sensitive and after 6 weeks of therapy she was AFB negative. However, given the extent of her disease it was recommended she have 9 months of treatment with dual therapy, isoniazid and rifampicin.