
- 46 yr old male patient was brought to the Emergency Department with a sudden episode of loss of consciousness. Attenders gave the history of generalized tonic–clonic movements, associated with up-rolling of the eyes, tongue bite, and urinary incontinence. This was followed by unresponsiveness after which the attenders rushed to emergency.
- There is a history of multiple similar episodes in the past and the patient was not taking any treatment for the same.
- There was fracture in the left wrist along with dislocation of thumb.
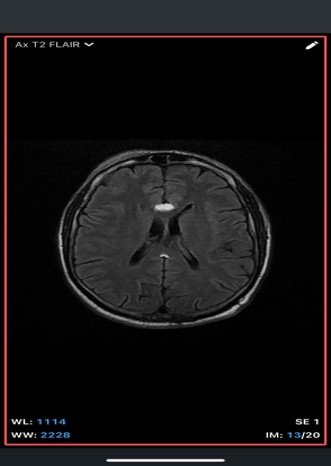
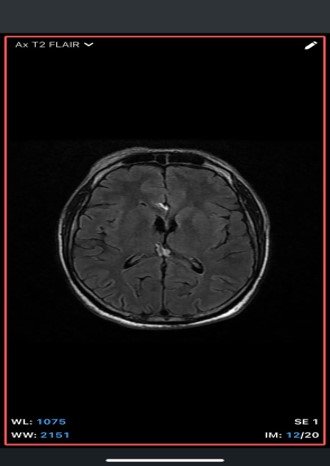
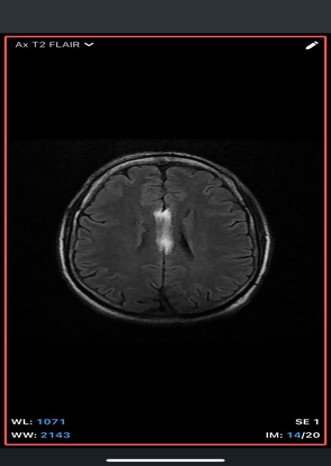
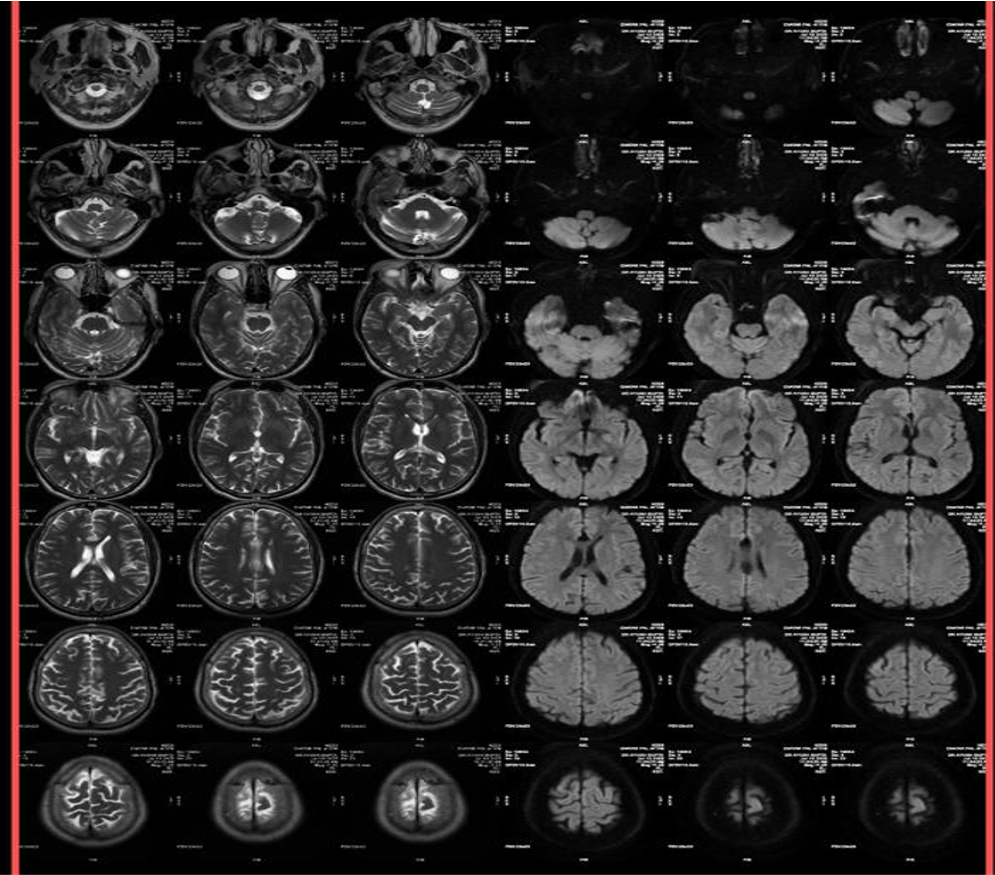
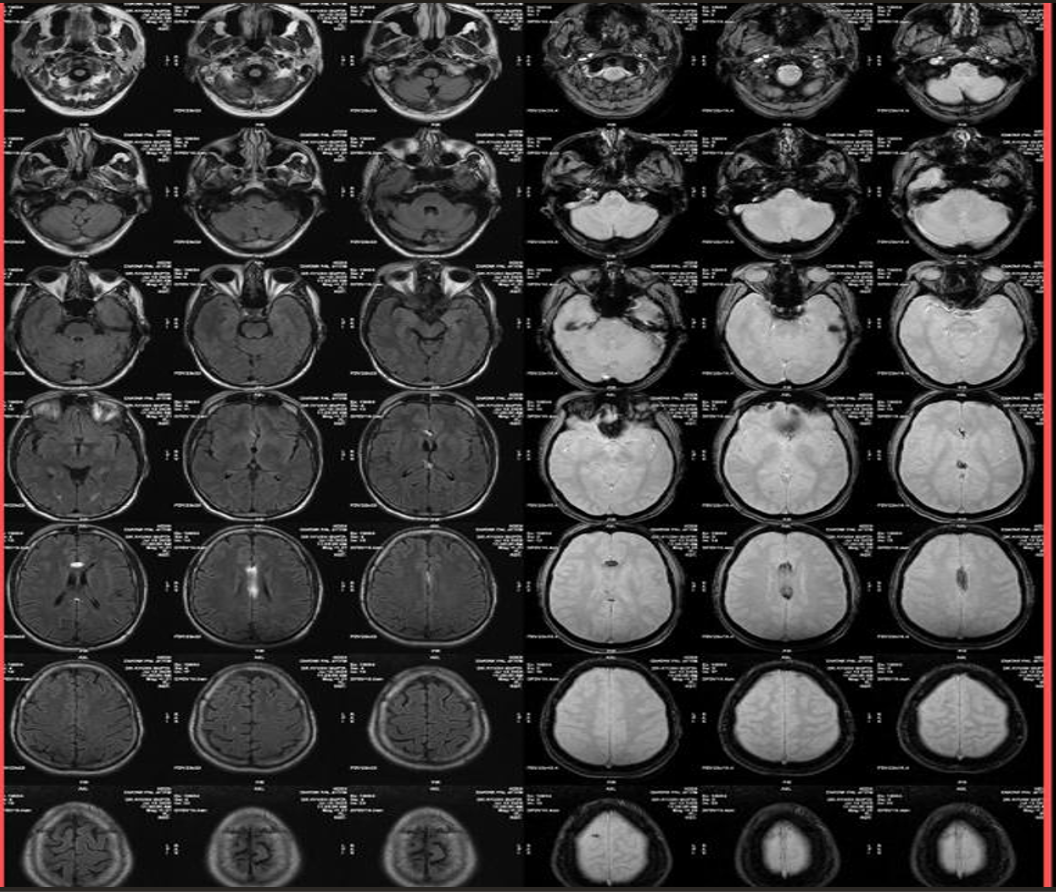
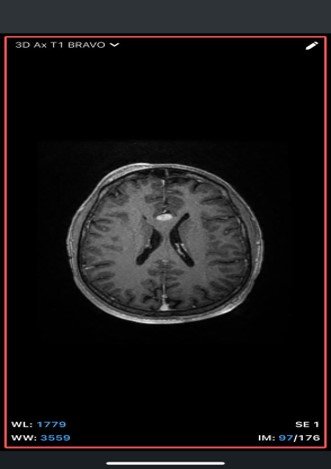
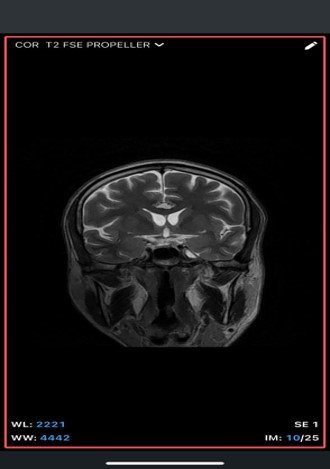
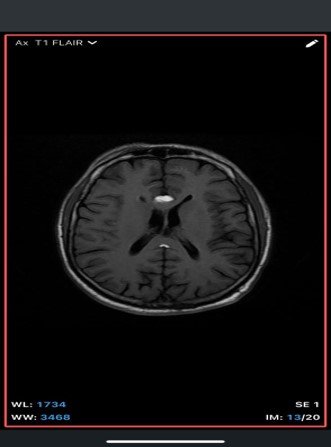
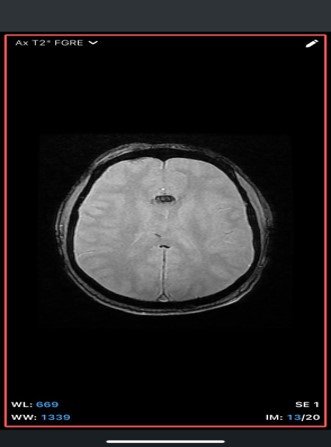
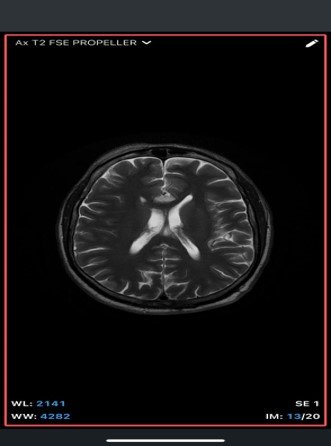
An extra-axial TI/T/Flair hyperintense lesion in midline at the inferior edge of the interhemispherie fissure extending along the superior margins of the corpus callosum with areas of blooming consistent with calcification and no post contrast enhancement –likely pericallosal lipoma.

Intracranial dermoid cyst
- fat-containing, usually midline.
- May rupture, causing fat droplets in subarachnoid space.
- On MRI: fat signal similar to lipoma, but often lobulated with mixed intensity due to hair, keratin, and calcifications
Teratoma (mature)
- Contains fat, calcification, and sometimes teeth/bone.
- More heterogeneous than lipoma on MRI.
- Often associated with mass effect.
Fat-containing glioma or other neoplasm
- Certain tumors (e.g., oligodendroglioma, ependymoma) may rarely contain fat or lipidized cells.
- Usually not as homogeneous as lipoma and often enhance with contrast.
Calcified midline tumors or malformations
- Oligodendroglioma, pineal region tumors, or meningioma can have calcifications and mimic lipoma in non-fat-suppressed images.
- CT helps differentiate fat from calcification.
Lipomatous hypertrophy of the corpus callosum
- Fat deposition within the corpus callosum itself, though extremely rare.
- MRI shows diffuse, infiltrative high T1 signal without a discrete capsule.
A rare, congenital, benign lesion composed of mature adipose tissue located within the pericallosal cistern, closely related to the corpus callosum. It is a developmental anomaly rather than a true neoplasm.
Epidemiology
- Represents <0.1–0.5% of all intracranial tumors.
- Common location: Along the corpus callosum, particularly pericallosal region.
- No significant sex predilection.
- Often detected incidentally during imaging for seizures, headache, or other neurological complaints
Etiopathogenesis
- Originates from abnormal differentiation of the primitive meninx (mesenchymal derivative of neural crest cells) during embryogenesis.
- Normally, the primitive meninx should resorb and be replaced by subarachnoid space. Failure of resorption results in persistence and differentiation into adipose tissue.
- Frequently associated with corpus callosum anomalies (agenesis, hypogenesis, or dysgenesis), which develop from the same embryonic midline structures.
Clinical Features
- Many patients are asymptomatic.
- When symptomatic:
- Seizures (most common presenting complaint, often generalized tonic–clonic)
- Headache
- Cognitive impairment or developmental delay (especially in children with associated callosal agenesis)
- Rare: focal neurological deficits, behavioral changes
- Symptoms usually result from associated malformations rather than the lipoma itself.
Imaging Findings-
- CT
- Well-defined, homogeneous, hypodense lesion (-50 to -100 HU, consistent with fat).
- May show peripheral or central calcifications (~50% cases).
- No enhancement with contrast.
- MRI
- T1-weighted: Hyperintense (fat signal).
- T2-weighted: Variable, usually hyperintense; may show chemical shift artifacts.
- Fat-suppressed sequences: Complete signal suppression confirms fat composition.
- Post-contrast: No enhancement.
- Often associated with:
- Corpus callosum agenesis/dysgenesis
- Interhemispheric cysts
- Calcifications (better on CT)
Management
- Asymptomatic cases:
- No surgical intervention (lesions are highly vascular and adherent to surrounding neurovascular structures → high risk).
- Symptomatic cases:
- Symptom-directed therapy (antiepileptic drugs for seizures).
Neurosurgical intervention only if secondary complications (very rare).