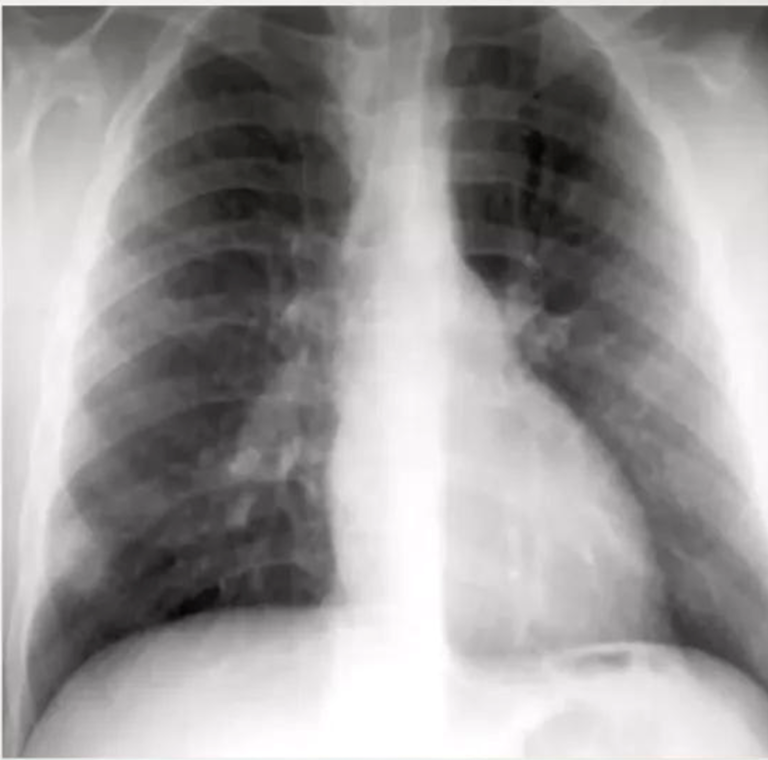
The most common abnormality in children is lymph node enlargement, which is seen in 90-95% of cases.
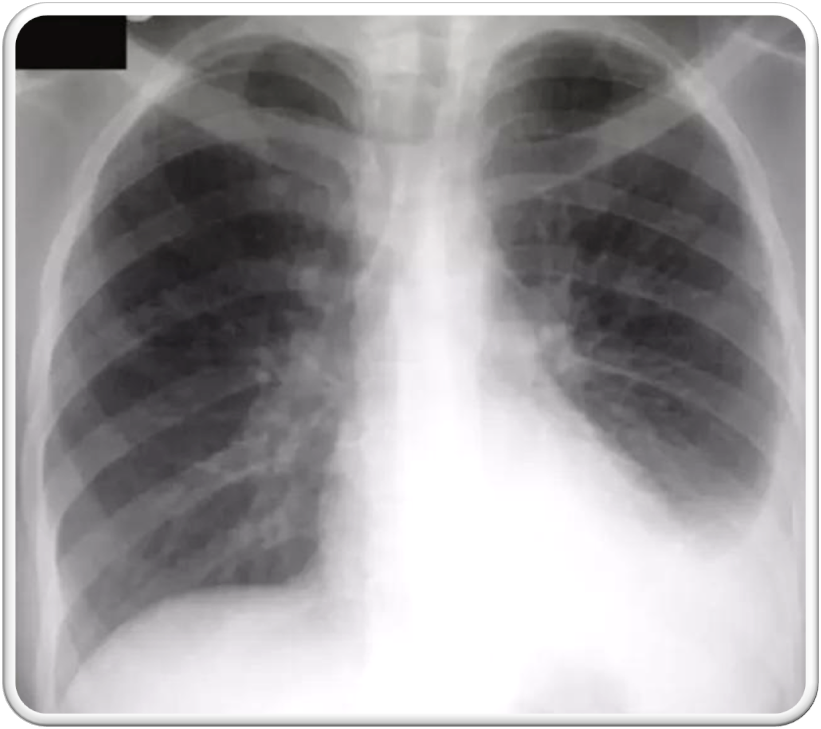
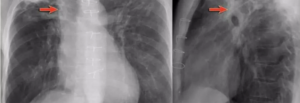
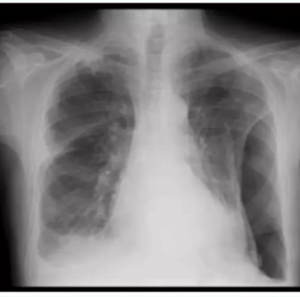
10-year-old child with tuberculosis, shows widening of the right paratracheal stripe
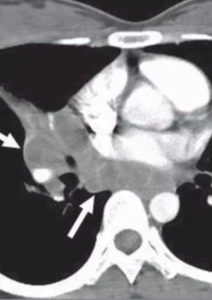
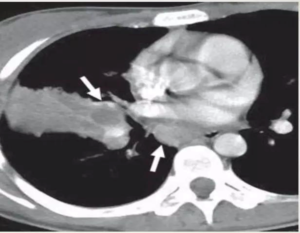
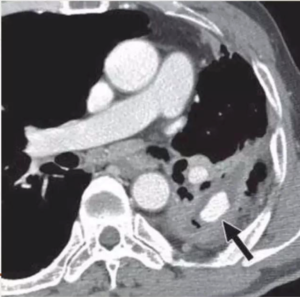
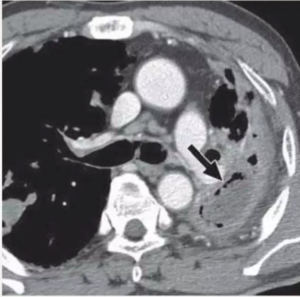
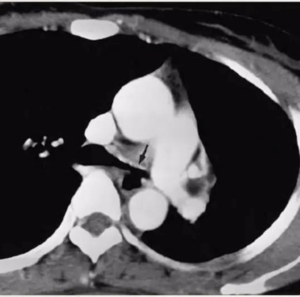
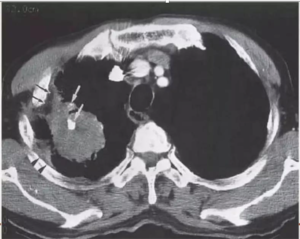
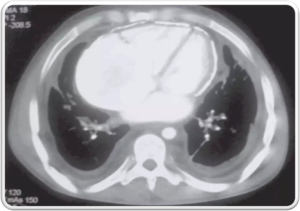
CECT show tuberculous nodes that show central areas of low attenuation suggestive of caseous necrosis and peripheral rim enhancement.
TUBERCULOUS NODE
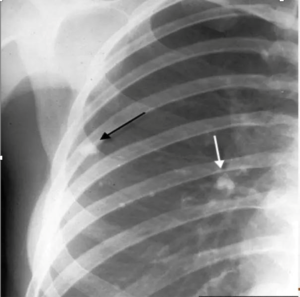
Ghon focus may be visualized on the chest radiograph as an airspace opacity
• Small tan-yellow subpleural granuloma in the mid-lung field on the right.
• Over time, the granulomas decrease in size and can calcify, leaving a focal calcified spot on a chest radiograph that suggests remote granulomatous disease.
typical of primary tuberculosis in a child
Parenchymal involvement is more in adults.
The combination of calcific lesions of the lung and lymph node is referred to as the “Ranke complex”
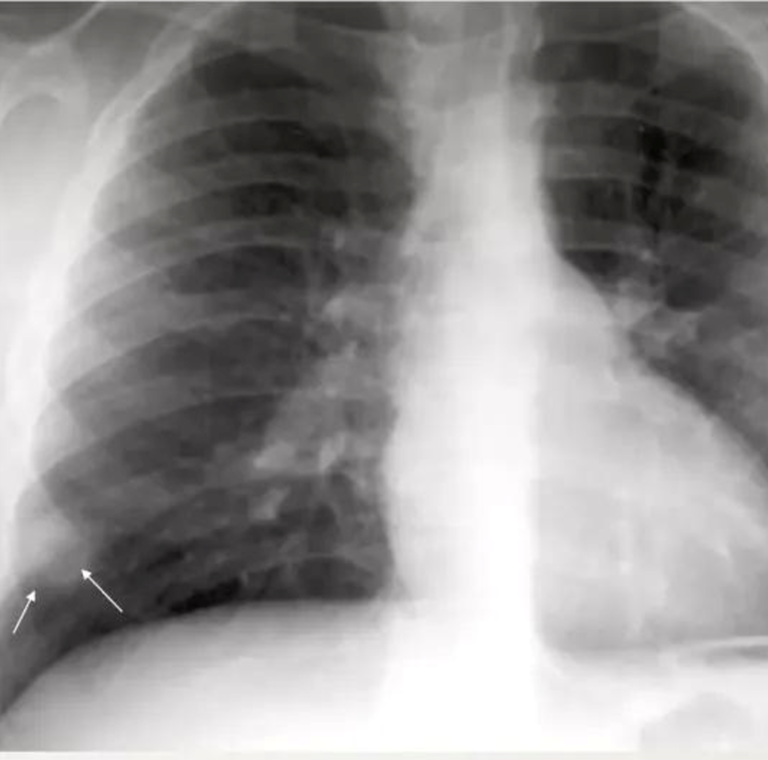
Airspace consolidation is usually unilateral, is evident radiographically in approximately 70% of children with primary TB.
obtained at level of right middle lobar bronchus
Pleural effusion is usually unilateral and due to subpleural infection.
Pleural effusions are more common in adults with primary tuberculosis (40%).
shows a right upper lobe airspace opacity adjacent to the trachea.
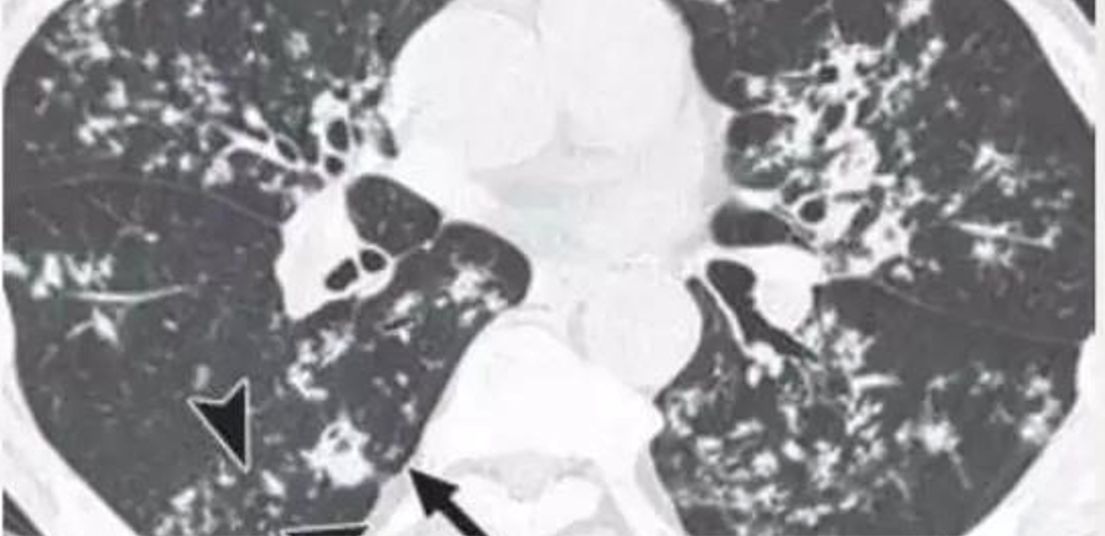
focal or patchy heterogeneous consolidation involving the apicoposterior segments of the upper lobes and the superior segments of the lower lobes
lateral view of the same patient, the typical location of the apicoposterior segment
The predilection for the upper lobes is thought to be due to decreased lymph flow in the upper regions of the lung.
An alternative explanation is the presence of higher oxygen tension in that region.
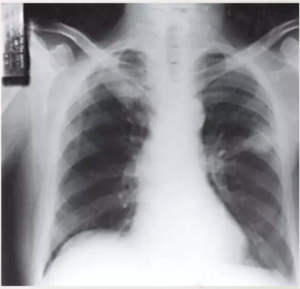
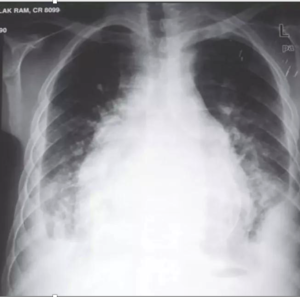
Xray showing cavitatory consolidation in right upper lung zone and multiple ill-defined nodules in both lungs
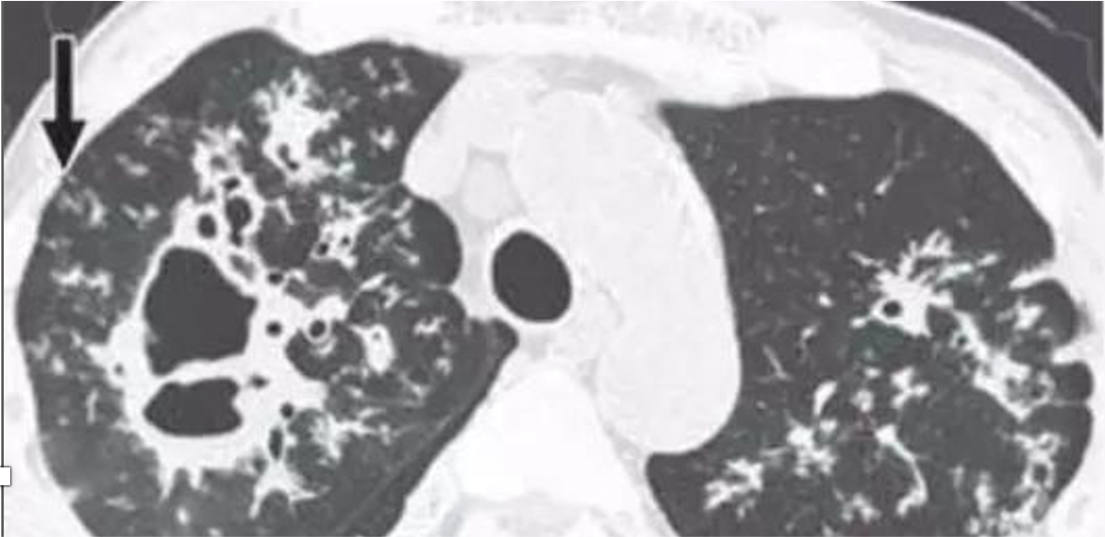
CAVITATION AND TREE IN BUD SIGN IS INDICATIVE OF AN ACTIVE DISEASE PROCESS AND USUALLY HEALS S A LINEAR OR FIBROTIC LESION.
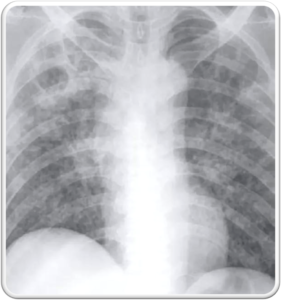
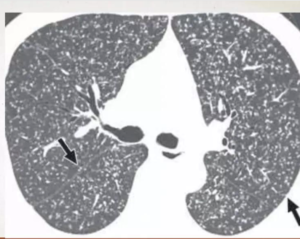
Miliary TB refers to widespread dissemination of TB by hematogenous spread.
Seen more frequently in reactivation TB.
The characteristic radiographic and high-resolution CT findings consist of innumerable, 1- to 3-mm diameter nodules randomly distributed throughout both lungs
The characteristic radiographic and high-resolution CT findings consist of innumerable, 1- to 3-mm diameter nodules randomly distributed throughout both lungs
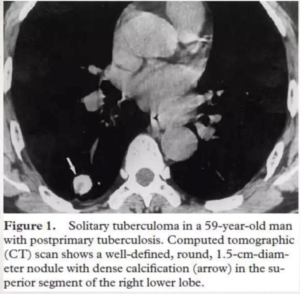
Sequelae of healed primary TB, but may be seen in 3-6 percent of cases of post primary tuberculosis as the main or only abnormality
calcified nodule consistent with a calcified granuloma. In addition, there is bilateral apical pleural thickening
TUBERCULOUS EMPYEMA
TUBERCULOUS EMPYEMA
Empyema may also communicate with the bronchial tree by bronchopleural fistula and can show an air fluid level
RASMUSSEN ANEURYSM
Rasmussen aneurysm is a pseudoaneurysm that results from weakening of the pulmonary artery wall by adjacent cavitatory TB.
CECT obtained shows cavitatory consolidation with air-crescent sign in left upper lobe.
Pneumothorax occurs in approximately 5 percent of patients with postprimary TB, usually in severe cavitatory disease.
Bacilli can enter the pleural space from a juxtapleural caseating granuloma, or via hematogenous dissemination
Tuberculosis may predispose to the development of bronchogenic carcinoma by local mechanisms (scar cancer)
Carcinoma may lead to reactivation of TB, both by eroding into an encapsulated focus and by affecting the patient’s immunity.
PERICARDITIS
Tuberculosis may predispose to the development of bronchogenic carcinoma by local mechanisms (scar cancer)
Carcinoma may lead to reactivation of TB, both by eroding into an encapsulated focus and by affecting the patient’s immunity.