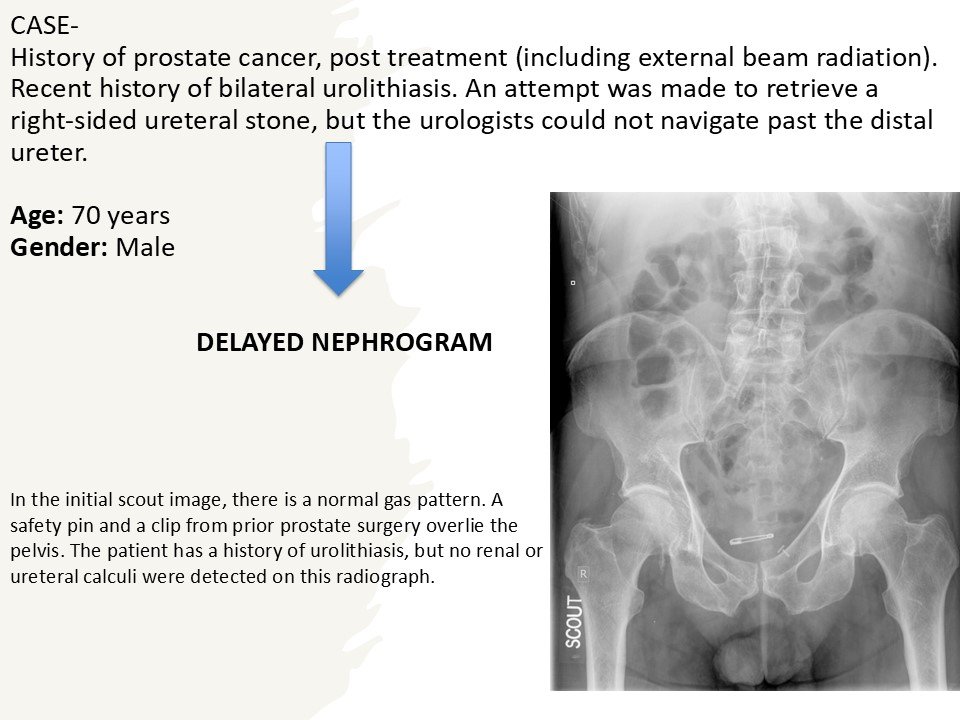
Delayed nephrogram(if contrast phase is done later).
Non-contrast axial CT image showing renal stone.
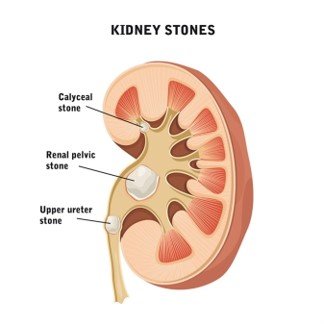
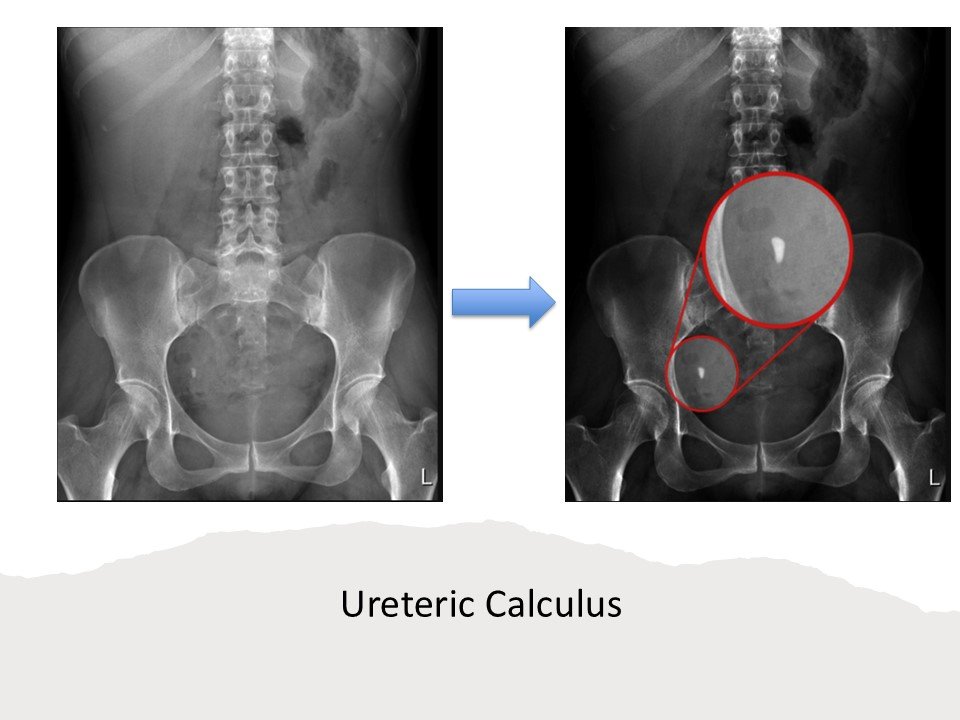
Ureteric Calculus:
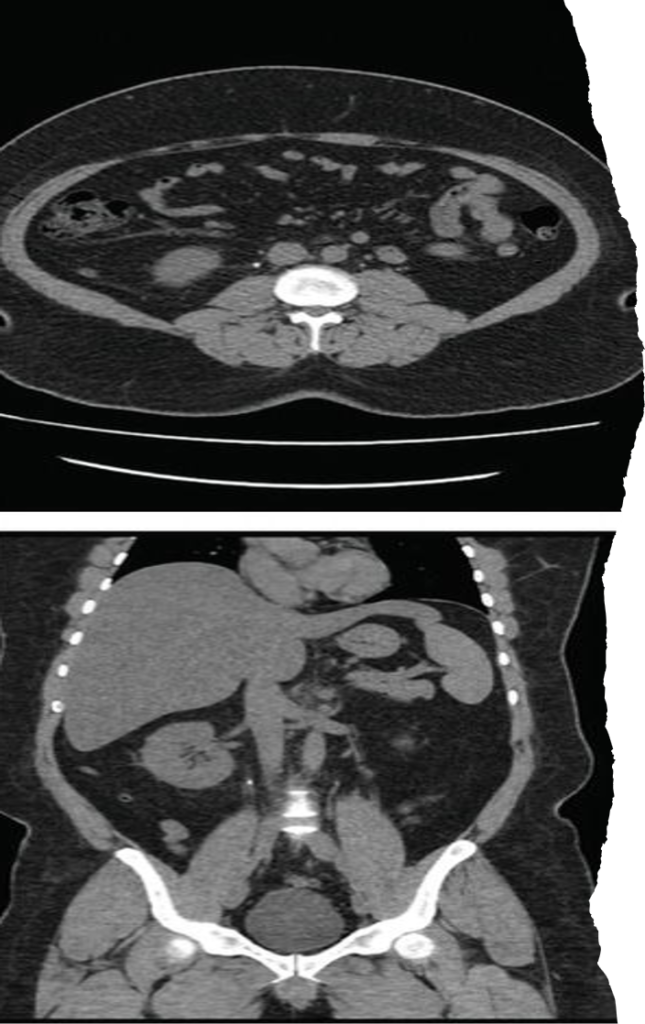
CT KUB axial and coronal sections demonstrating an obstructing right proximal ureteric calculus.
1)Hyperdense focus along ureteric course.
2)Soft-tissue rim sign favors stone over phlebolith.
3) Associated with Upstream hydroureter & hydronephrosis.
CT KUB axial and coronal sections demonstrating a left renal pelvis calculus (a and b) and left distal ureteric calculus (c).
Plain CT KUB showing right staghorn and giant bladder calculus measuring 9.5 × 9.4 × 11.1 cm³.
Large branching calculus occupying renal pelvis and calyces.
Usually composed of struvite.
Associated with recurrent UTI.
Suggests long-standing disease.
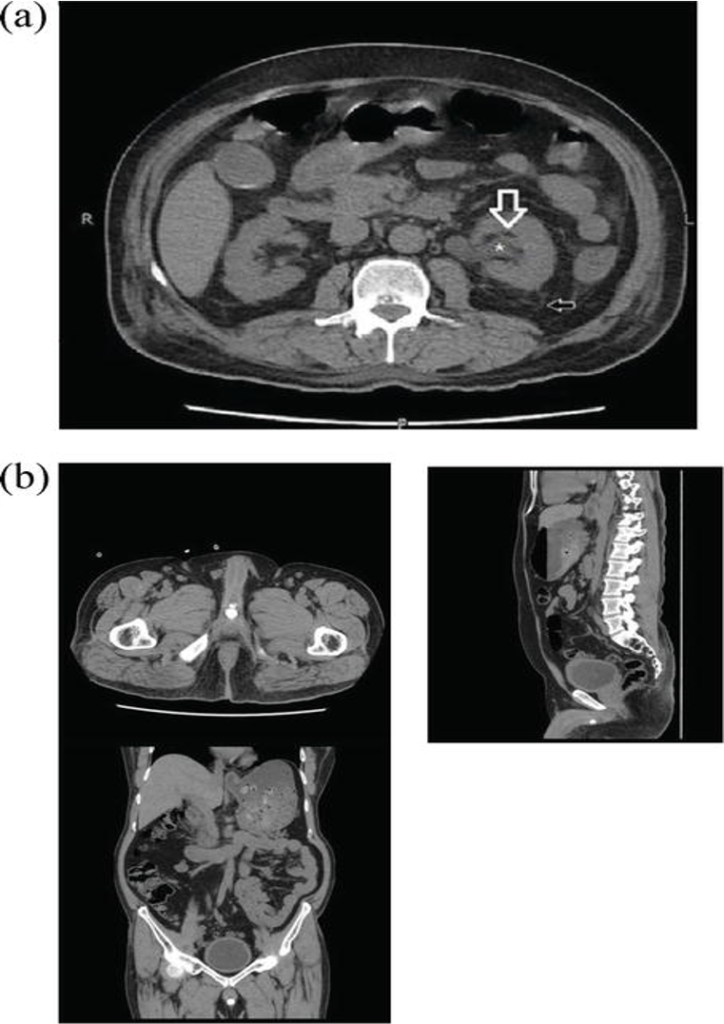
View of perirenal fat stranding in non-contrast computed tomography.
(a) Hydronephrosis (*), reduced peripelvic fat (white arrow) and increased perinephric fat stranding (black arrow) as compared to contralateral side.
(b) CT KUB axial, sagittal and coronal sections demonstrating multiple calcific densities near the bulbar urethra likely representing urethral diverticulum with stone formation.
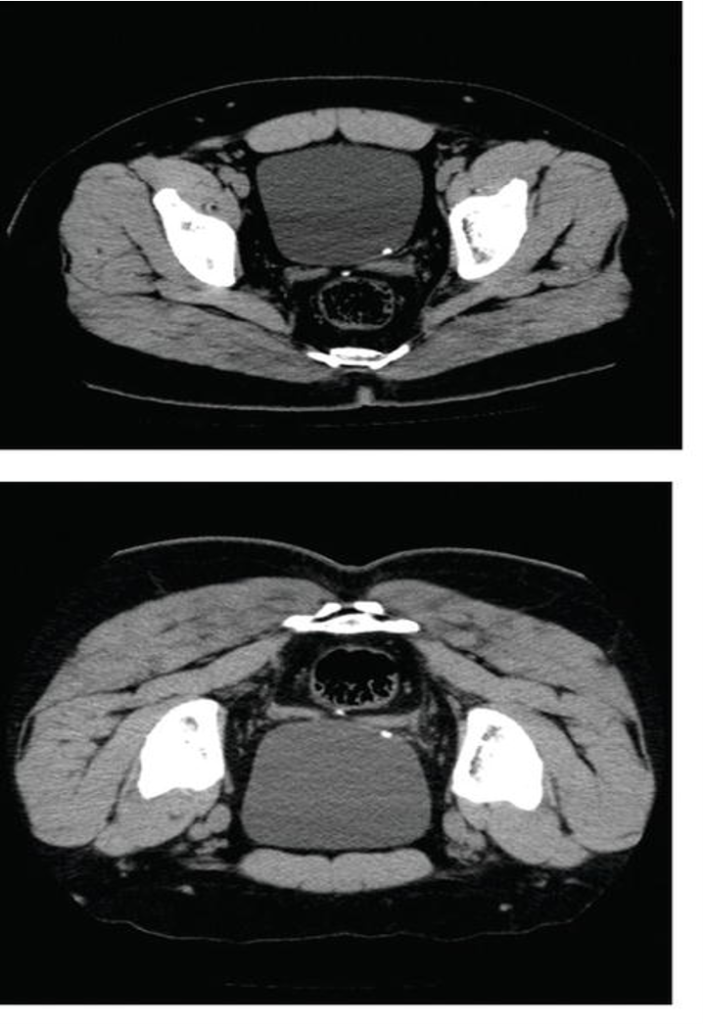
CT KUB axial, coronal and sagittal sections demonstrating a calculus in the prostatic urethra.
CT KUB axial supine and prone positions demonstrating a left-sided VUJ calculus.
Advantages
Highest sensitivity and specificity.
Detects radiolucent stones.
Provides anatomical and etiological diagnosis.
Limitations
Radiation exposure.
Avoid in pregnancy.
Drug stones (indinavir) may be CT-lucent.
Ultrasound (USG KUB)
Advantages
Highest sensitivity and specificity.
Detects radiolucent stones.
Provides anatomical and etiological diagnosis.
Limitations
Radiation exposure.
Avoid in pregnancy.
Drug stones (indinavir) may be CT-lucent.
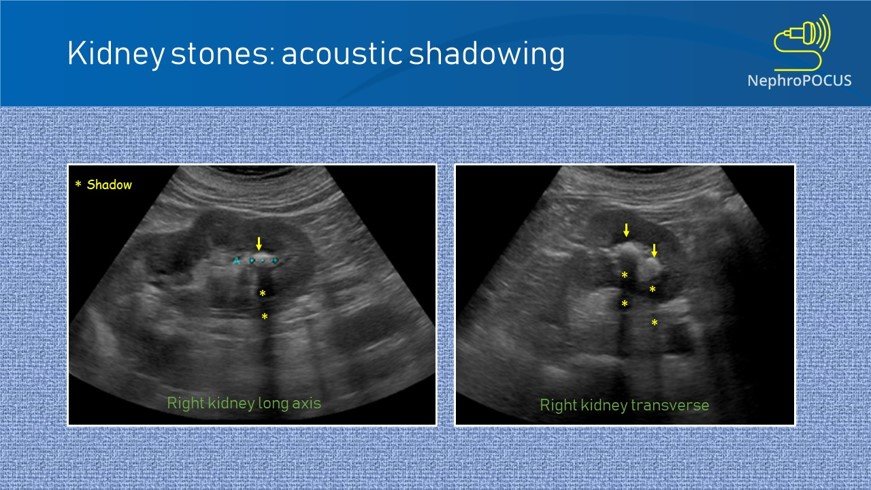
The bright echogenic focus marked by the arrow represents a renal calculus.
Behind this echogenic focus, there is a posterior acoustic shadow (dark vertical band), which is a key diagnostic feature of a stone.
Left renal stone is seen as an echogenic focus with posterior acoustic shadowing. No dilatation of the renal cavities.
Advantages
No radiation exposure.
First-line investigation in pregnancy and pediatric patients.
Good sensitivity for renal stones.
Limitations
Poor visualization of mid-ureter.
Operator dependent.
Normal USG does not exclude ureteric calculus.
Early obstruction may show no hydronephrosis.
Stone Appearance
Stone Appearance
Radiopaque stones appear as dense white opacities.
Visibility depends on stone composition and size.
Stones Seen:
Calcium oxalate, phosphate, struvite.
Stones Not Seen:
Uric acid, xanthine, matrix stones.
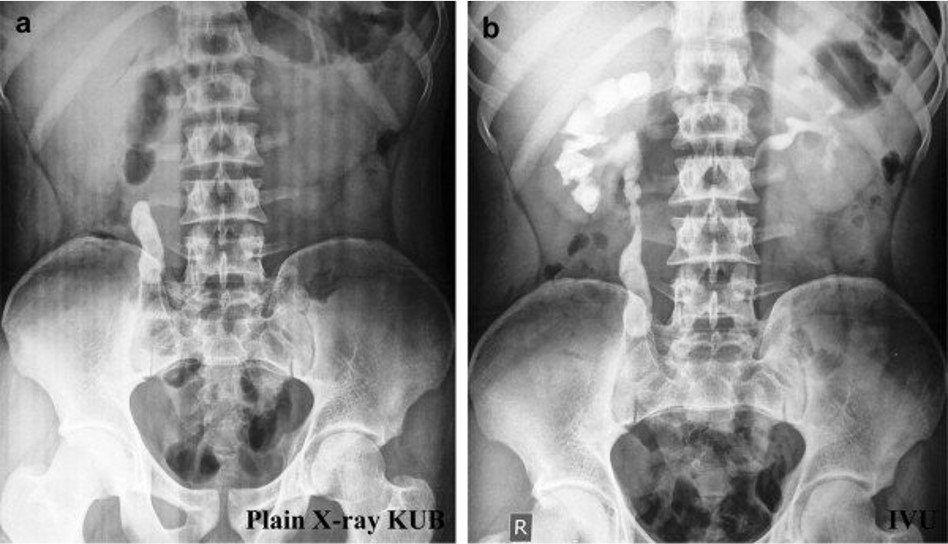
a) Plain X-ray KUB showing a large radio-opaque density in the region of Right upper ureter, b) IVU shows presence of right upper ureteric calculus with prompt uptake and excretion of contrast from both renal units.
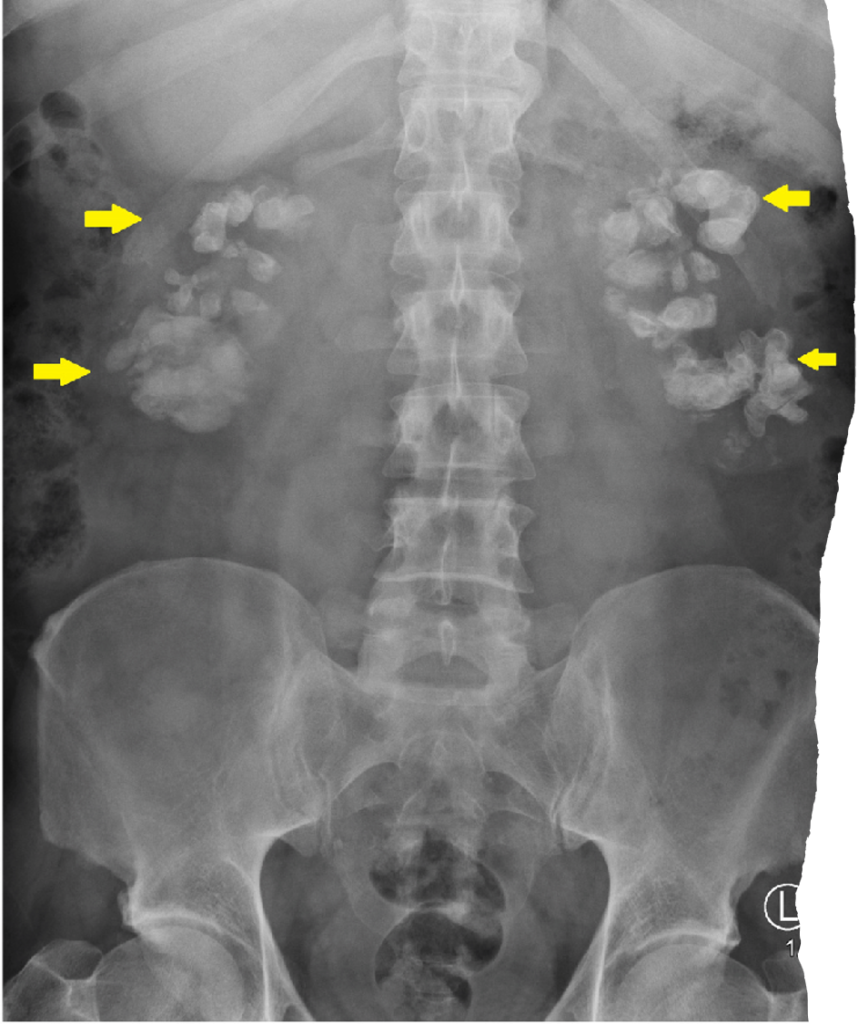
Staghorn Calculus
Large branching radiopacity occupying renal area.
Matches collecting system outline.
Suggests chronic infection and long-standing obstruction.
There is well defined branching radio-opaque calcific density superimposed over the pelvis and calyces of the left kidney.
x-ray KUB of the abdomen. Significant bilateral calcifications are shown to be projected over each kidney.
X-ray shows multiple round, calcified densities with radiolucent centers in the pelvis.
Uses:
Baseline documentation of radiopaque stones.
Follow-up to assess stone migration or clearance.
Often combined with USG to improve detection.
Differentiation:
Phlebolith shows central lucency (donut sign).
Lies lateral to ureteric course.
Limitations:
Cannot assess obstruction or renal function.
Overlap with bowel shadows may cause false positives.
Intravenous Pyelogram (IVP)
Stone Findings:
Filling defect in contrast-filled collecting system.
Delayed contrast excretion from affected kidney.
Obstructive Changes:
PCS dilatation.
Clubbing of calyces.
Hydroureter.
IVP showing the filling defects in the left ureter of the patient.
ØIVP showing the filling defects in the right ureter of the patient.
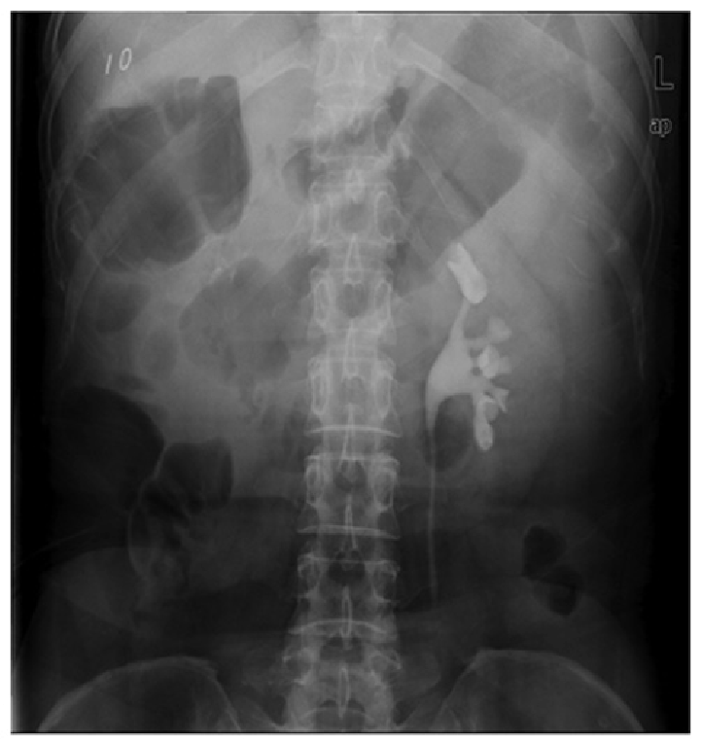
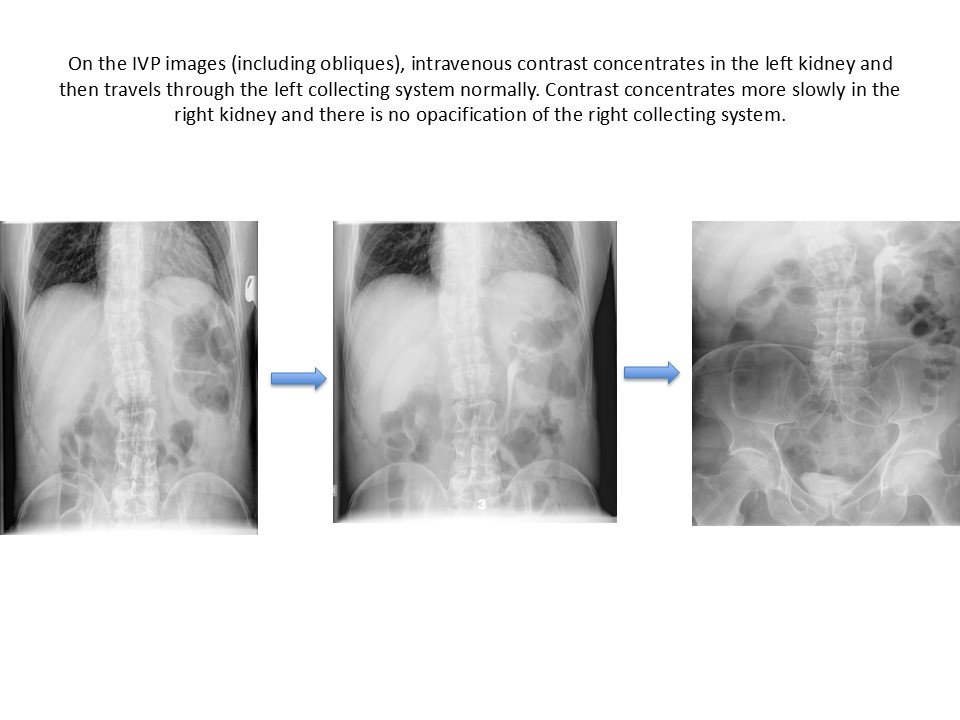
The right kidney and ureter were not visualized on intravenous urography until 60 min. The left kidney and ureter revealed normal.
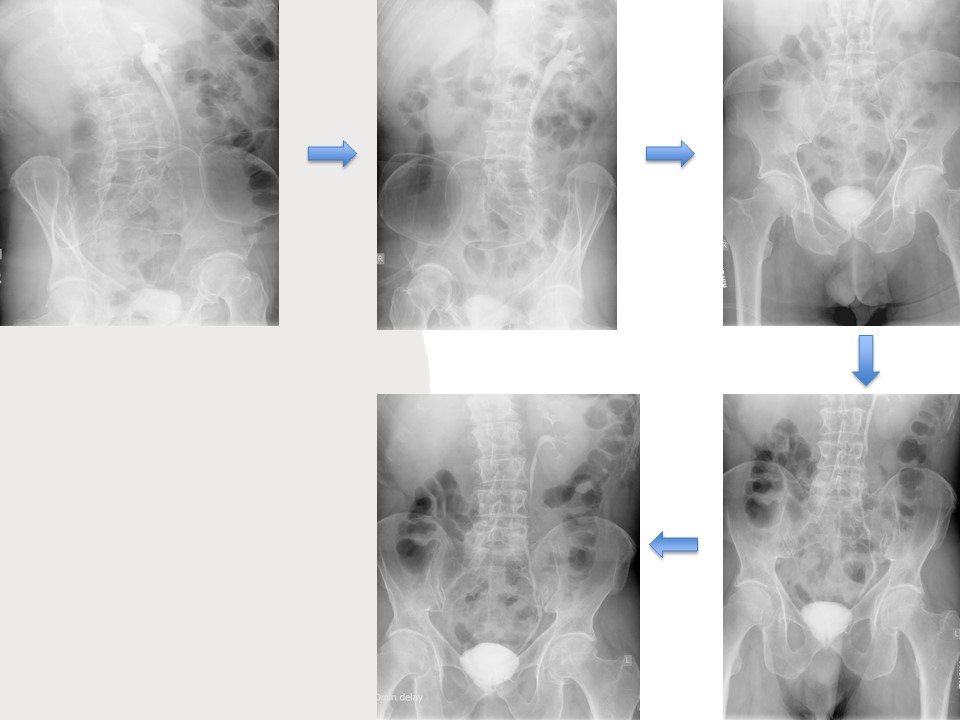
On the 20 min post-void image there is opacification of the right kidney (delayed nephrogram), still without any contrast in the collecting system, compatible with high-grade obstruction of the right collecting system.
Severe Obstruction:
Non-visualized kidney.
Functional Role:
Demonstrates renal excretory function.
Delayed nephrogram suggests acute obstruction.
Current Status:
Largely obsolete.
Replaced by CT urography.
Limitations:
Contrast nephrotoxicity.
Contraindicated in renal failure and contrast allergy.
Final Take-Home Points
NCCT KUB → investigation of choice for renal colic