Degenerative osteophytes compress the spinal cord.
Reduced AP diameter of spinal canal.
Cord flattening seen.
T2 hyperintensity indicates myelomalacia.
Most common cause of compressive myelopathy.
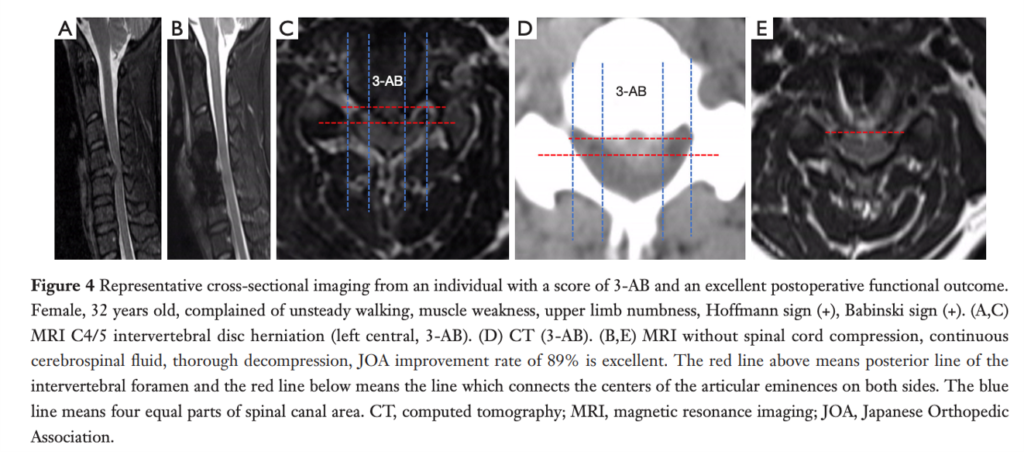
A sagittal T2-weighted magnetic resonance imaging of cervical spondylotic myelopathy patient shows the change of spinal cord signal intensity.
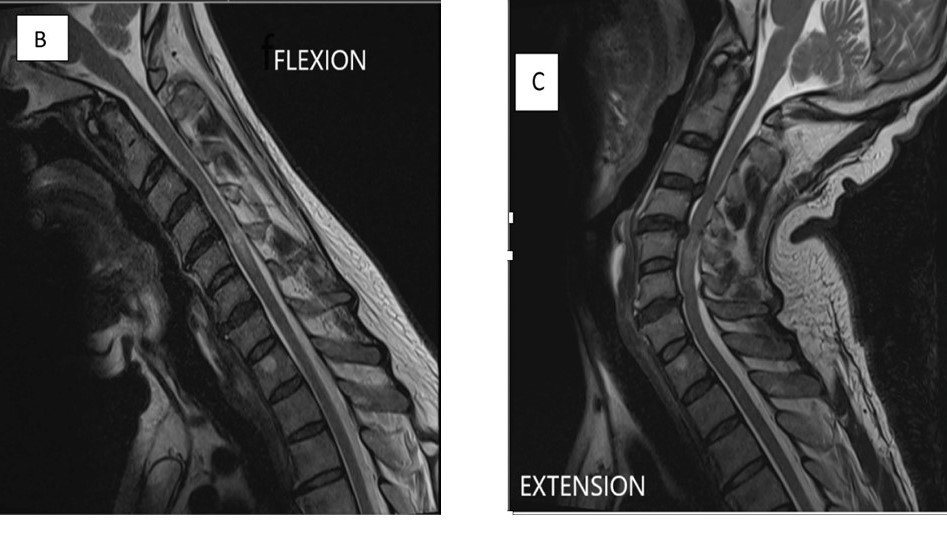
CASE- A 64-year-old man developed neck pain after falling off a truck one week ago. T1- and T2-weighted sagittal MR images (1 and 2) are provided. What are the findings? What is your diagnosis?
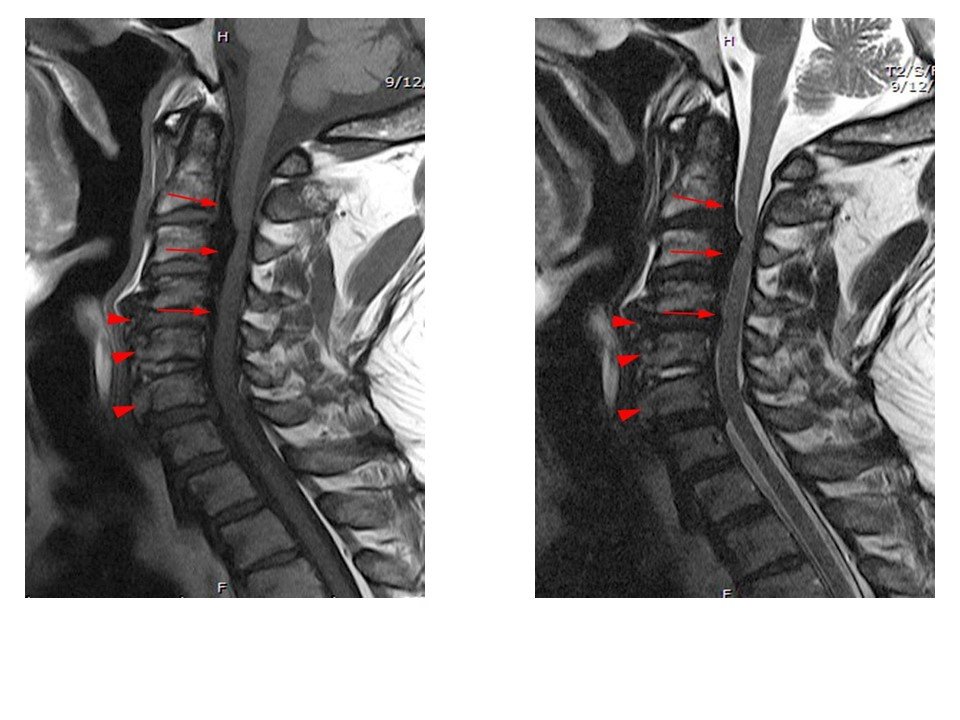
An extensive low signal intensity epidural abnormality posterior to the vertebral bodies and discs from C2 through C6 (arrows) produces spinal stenosis, most severe at C3, where there is resultant cord compression and faint T2 cord signal hyperintensity. Ossifications are present anterior to the vertebral bodies and discs (arrowheads).
Thick ossification is present posterior to the vertebral bodies and discs corresponding to the MR low signal intensity (arrows). Flowing ossification is present along the anterior vertebral bodies and discs (arrowheads).
ANSWER- Ossification of the posterior longitudinal ligament (OPLL), continuous type, producing spinal stenosis, cord compression and edema. Diffuse idiopathic skeletal hyperostosis (DISH) is also present.
Ossification of posterior longitudinal ligament
Hypointense ossified ligament posterior to vertebral body.
Severe anterior cord compression.
Often multilevel involvement.
T2 hyperintensity suggests chronic cord injury.
Common in Asian population.
Epidural collection compressing the spinal cord.
Cord displaced and flattened.
T2 hyperintense cord edema.
Rim enhancement on contrast.
Neurosurgical emergency.
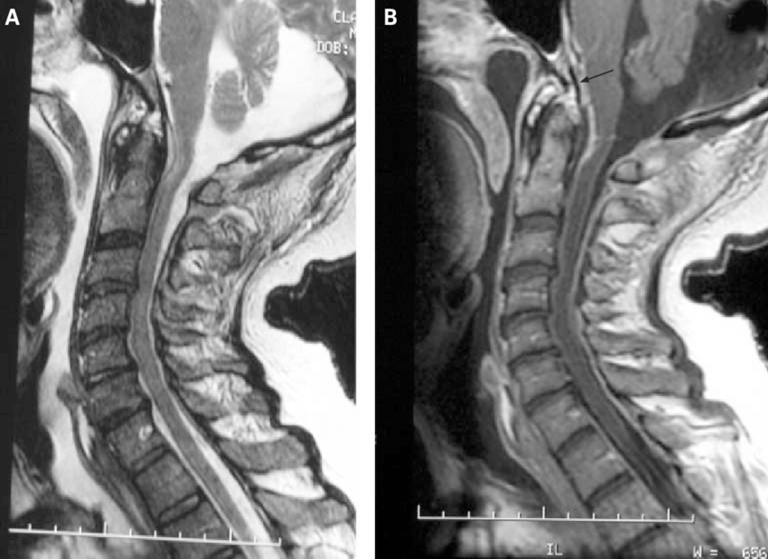
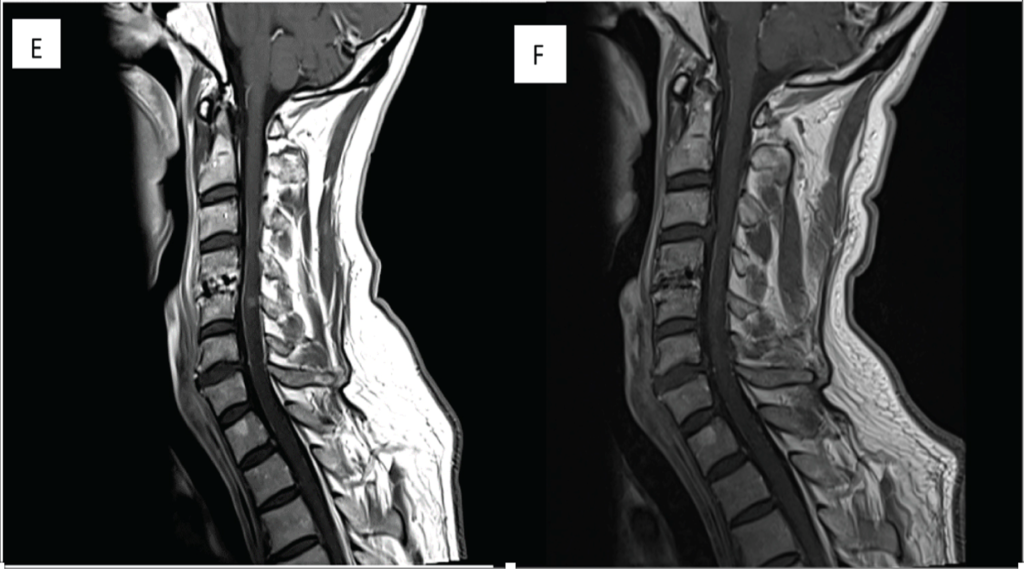
MRI of a patient with a spinal epidural abscess presenting with myelopathy. These abnormalities were initially missed when imaged without contrast and interpreted by general radiologists. (A) Sagittal T2 (fast spin echo) image demonstrating increased signal anterior to the cervical medullary junction at C1 and C2. (B) Sagittal T1 image with contrast, showing enhancement of the abscess, extending through the foramen magnum up to the clivus (arrow).
Thick ossification is present posterior to the vertebral bodies and discs corresponding to the MR low signal intensity (arrows). Flowing ossification is present along the anterior vertebral bodies and discs (arrowheads).
Mass lesion causing extrinsic cord compression.
Cord displaced from normal position.
T2 hyperintensity due to cord edema.
Enhancement seen on contrast MRI.
Includes metastasis, meningioma, schwannoma.
Preoperative MRI cervical spine T1W1 with contrast shows contrast enhancement at C4/C5 level.
Postoperative MRI cervical spine T1W1 with contrast at 6 months shows slight reduction in enhancement at C4/C5 level.
Postoperative MRI cervical spine T1W1 with contrast at 12 months shows almost complete resolution of enhancement at C4/C5 level.
Acute Transverse Myelitis
No external compression of spinal cord.
Long-segment intramedullary T2 hyperintensity.
Cord may appear swollen.
Central cord involvement common.
Patchy enhancement may be seen.
Intradural Lesions with a diagnosis of Transverse Myelitis. T2 hyperintensity lesion T8-T12 in a 20–24-year old participant who presented with progressive paraplegia over 3 weeks. A diagnosis of transverse myelitis was made and the patient improved on steroids.
Lesion extends over more than 3 vertebral segments.
Central gray matter involvement.
No cord compression.
Bright T2 signal.
Suggestive of NMO spectrum disorder.
Short-segment lesion (<2 vertebral segments).
Partial cord involvement.
No cord expansion.
Minimal or no enhancement.
Often associated with brain lesions.
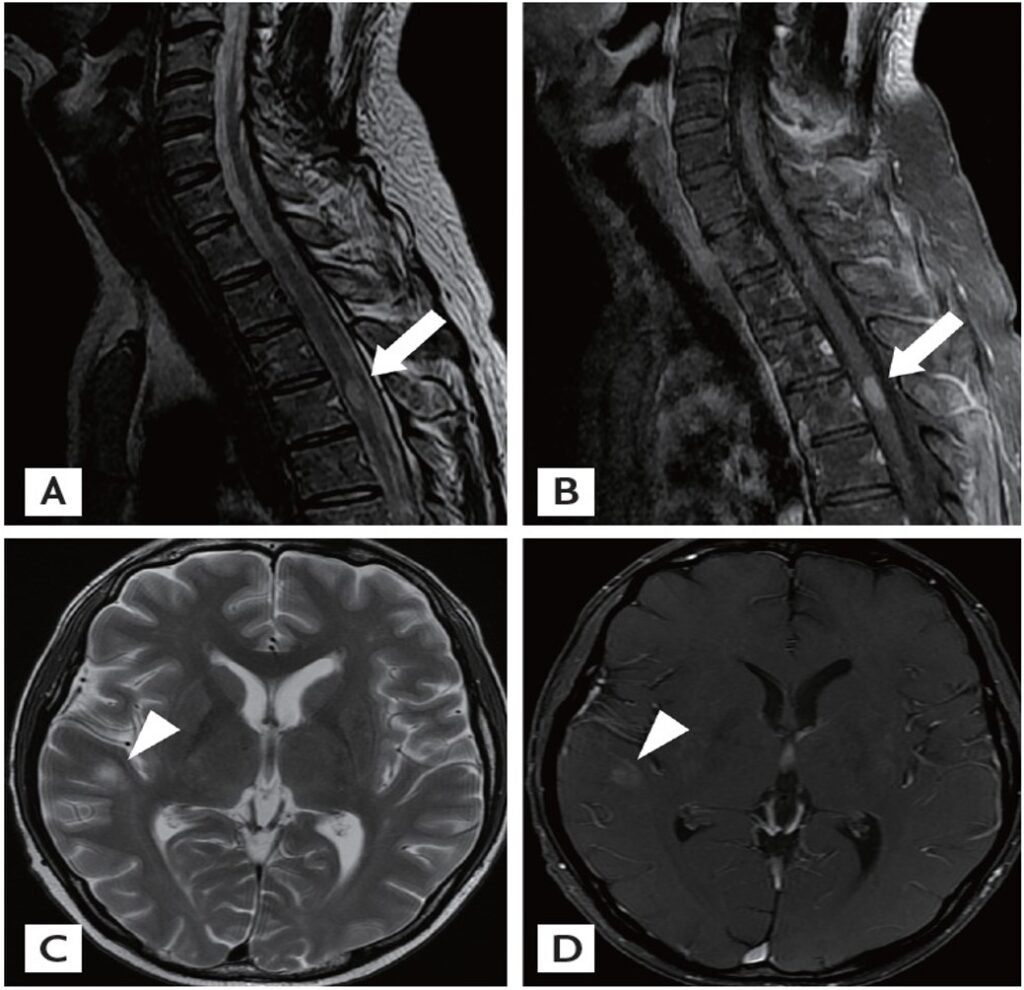
Magnetic resonance imaging (MRI) scans of the spine and brain. (A, B) Sagittal T2-weighted MRI of the thoracic cord demonstrates an intramedullary enhancing lesion at T3 (arrows). (C, D) Axial T2-weighted MRI of the brain shows round hyperintense lesions with slight enhancement in the right temporal subcortex (arrowheads).
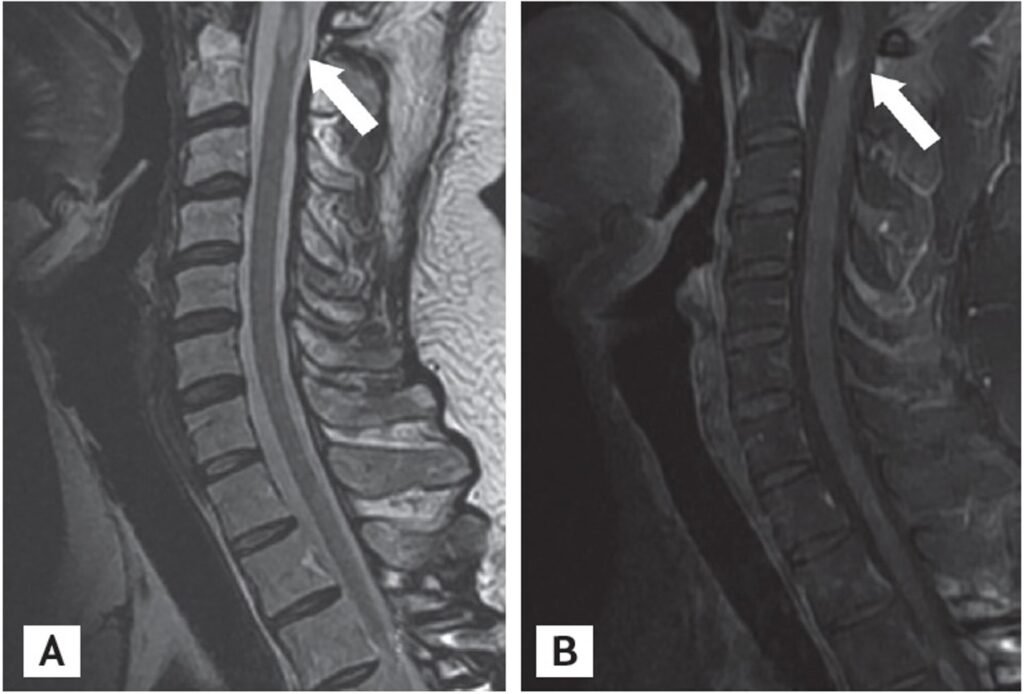
Magnetic resonance imaging (MRI) scans of the cervical spine (secondary bilateral lower leg weakness 3 years after allogeneic stem cell transplantation). (A, B) Sagittal T2-weighted MRI of the cervical cord demonstrates an intramedullary enhancing lesions at C1 and C2 (arrows). The previous enhancing lesion (at T3) disappeared.
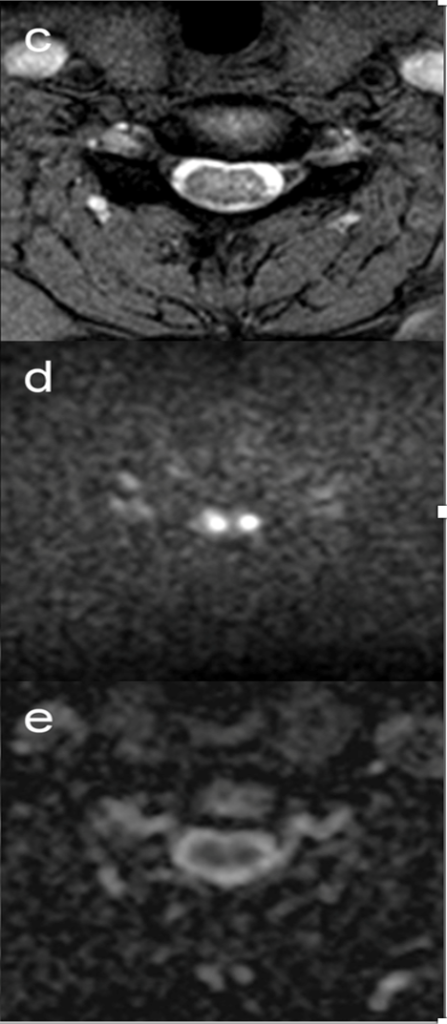
No external compression.
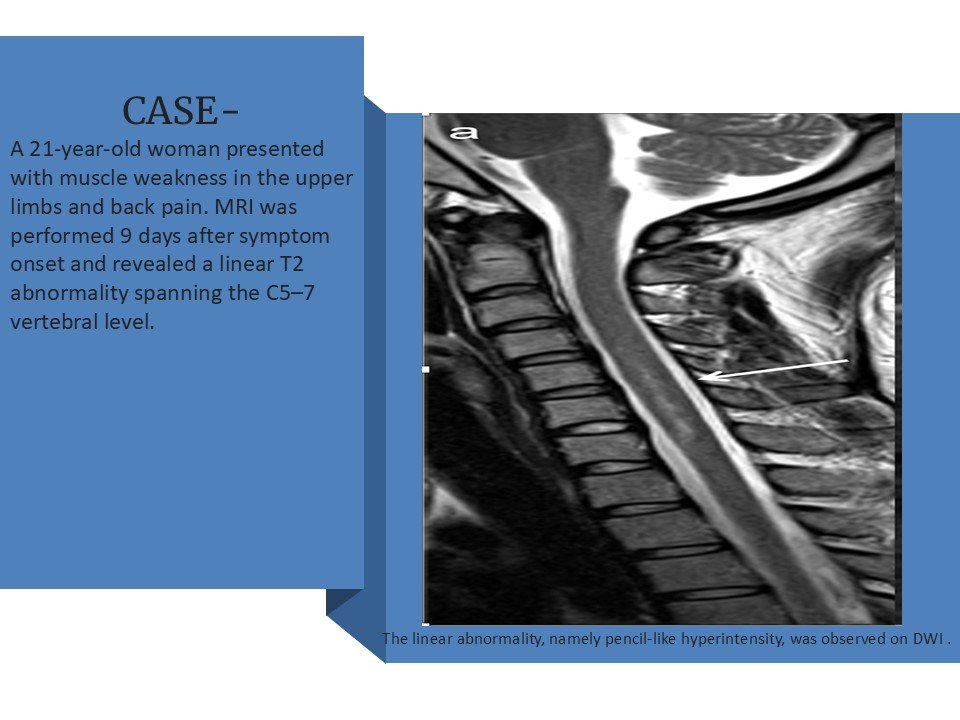
Pencil-like T2 hyperintensity.
Anterior spinal artery territory involved.
Restricted diffusion on DWI.
Acute onset clinically.
At the C5/6 intervertebral level (arrows, a and b), mild T2 hyperintensities around the anterior horns were observed on the axial plane.
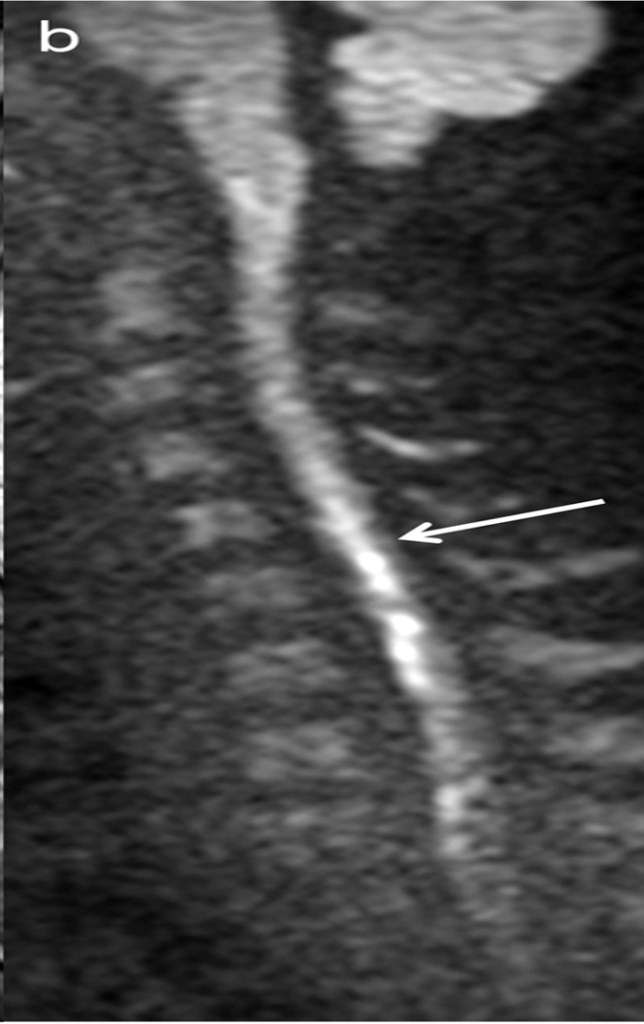
(c) The hyperintensities became a pair of apparent hyperintense lesions on DWI.
(d) Image corresponding to owl’s eyes sign. The lesions on the axial DWI were hypointense on ADC maps .
(e). She was diagnosed with spinal cord infarction. ADC, apparent diffusion coefficient; DWI, diffusion-weighted imaging; MRI, magnetic resonance imaging.
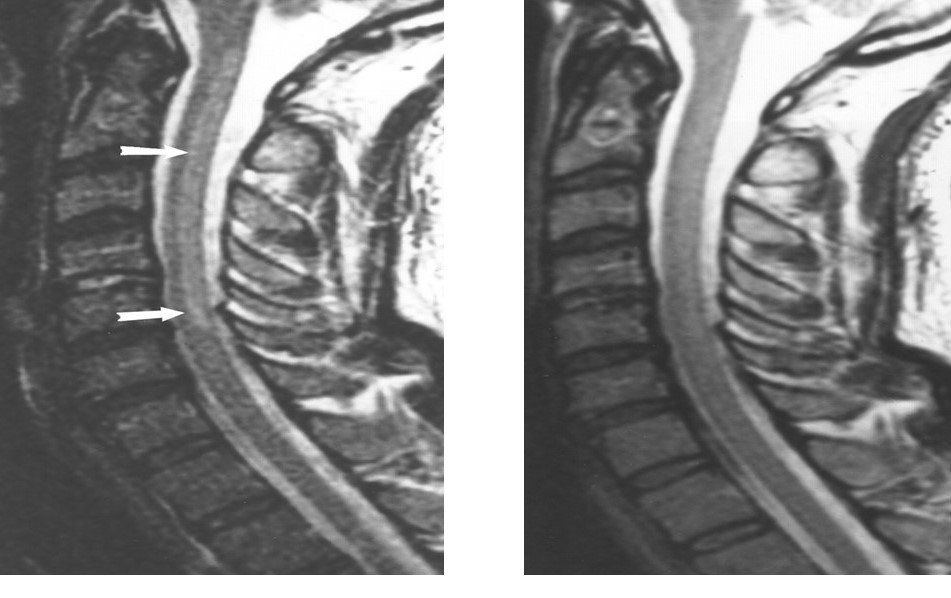
Symmetric posterior column T2 hyperintensity.
Inverted V sign on axial images.
No enhancement.
No cord compression.
Seen in vitamin B12 deficiency.
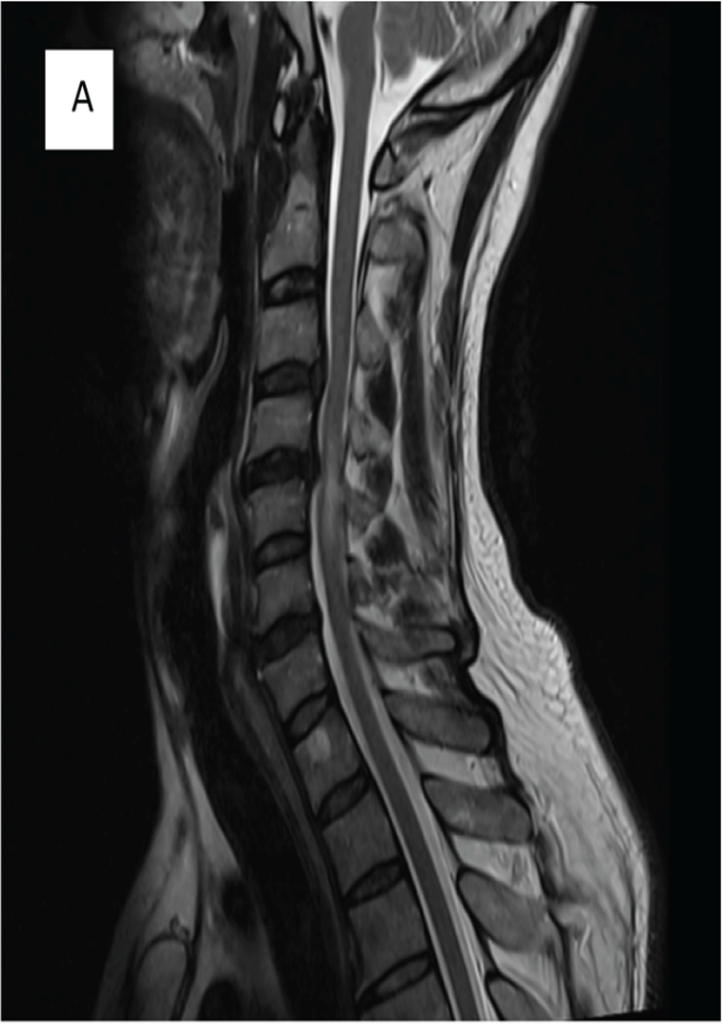
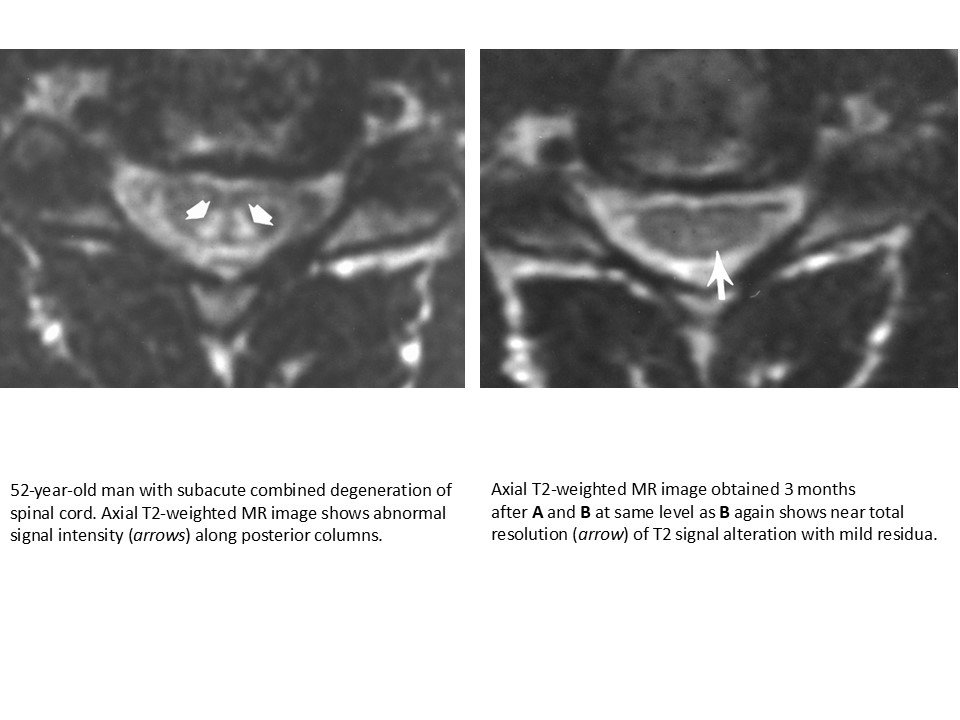
52-year-old man with subacute combined degeneration of spinal cord. Sagittal T2-weighted MR image shows abnormally increased signal intensity (arrows) along posterior columns of spinal cord extending from C1 through C6.
Follow-up sagittal T2-weighted MR image obtained 3 months after A and B shows near total resolution of signal abnormality.