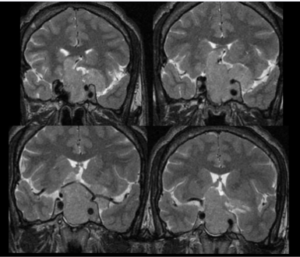
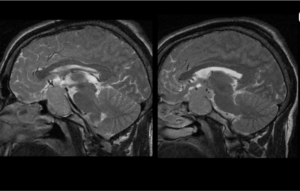
Sellar–suprasellar extension
Sagittal sections confirm that the mass extends from the sella into the suprasellar cistern
MRI Brain — Sagittal View
- Chiasmal involvement
The lesion abuts the floor of the third ventricle and elevates the optic chiasm — explaining the patient’s visual symptoms
- Posterior extent
No obvious extension into the posterior fossa or brainstem
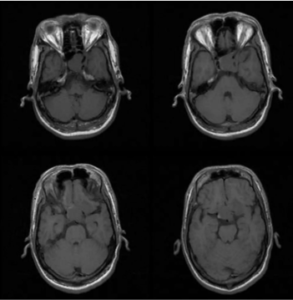
- On pre-contrast T1-weighted images, the sellar mass blends with adjacent brain parenchyma and is poorly conspicuous
- Following contrast administration, the lesion shows distinct heterogeneous enhancement that clearly outlines its margins — confirming a vascularised sellar mass