A 32-year-old female presented to the emergency department with 12 hours of headache, visual loss and difficulty speaking.
History :
- Headache was progressive and diffuse, worsening over the past several hours.
- She reports nausea and two episodes of vomiting.
- She noticed blurring of vision prior to the visual loss.
- No prior history of migraine or similar headaches.
- No recent trauma, infection, or drug use.
- Undergoing invitro fertilisation with hormone supplementation.
Neurological Exam:
- Clear mental status and a normal level of alertness.
- Intact upper/lower extremity motor and sensory function.
- No facial weakness or numbness.
- A right visual field cut (homonymous hemianopsia).
- Expressive and receptive aphasia.
- Normal gait without ataxia or unsteadiness.
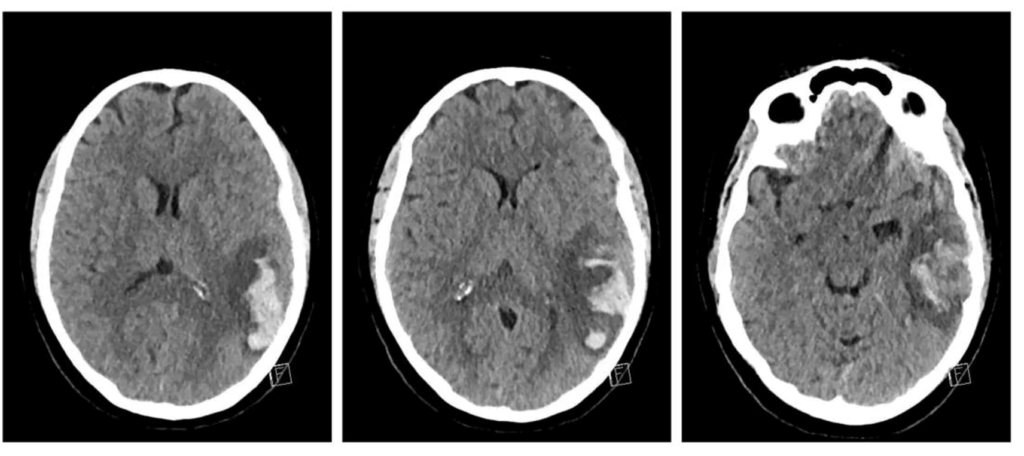
NCCT: Hemorrhagic infarct of left temporal lobe

This infarct is anatomically adjacent to two temporal lobe venous sinuses.
Case 2
A 31-year-old female with ulcerative colitis on Adalimumab and prednisone presented to the emergency department for headache, transient inability to move her right arm, and diminished sensation in the right hand.
History :
- Intermittent headache for one week; sudden worsening three hours prior to presentation.
- Inability to move right arm with onset of headache.
- Weakness resolved on presentation.
- Ongoing difficulty with fine motor movements of the right hand.
- Numbness over her 4th and 5th digits of her right hand.
- She is using a hormonal birth control patch.
Neurological Exam:
- Diminished sensation to the 4th & 5th right fingers; normal in all other dermatomes.
- 4/5 strength in entire right upper extremity; strength testing otherwise normal.
- Alert.
- No cranial nerve deficits.
- Normal cerebellar testing.
- Normal gait.
- Underwent non-contrasted head CT.
NCCT- Increased density in the anterior aspect of superior sagittal sinus and small frontal white matter haemorrhage
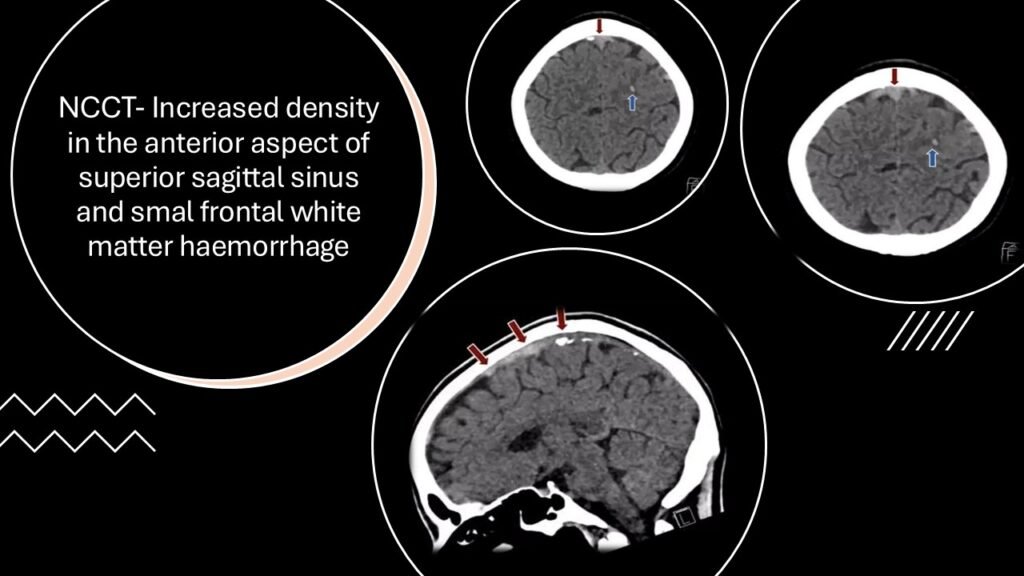

The area of hyperdensity corresponds to the location of superior sagittal sinus.
CEREBRAL VENOUS SINUS THROMBOSIS
Case 3
A 19-year-old female with recent admission for aseptic meningitis presented to the ED after a transient right-sided hemiparesis and a seizure-like episode, now reporting a headache.
History :
- The patient was admitted one month prior for aseptic meningitis from which she recovered.
- Sudden-onset right arm weakness when reaching for a container in the kitchen.
- Subsequently experienced right leg weakness, making it difficult to ambulate.
- The patient had a seizure-like episode on route to the hospital; which was witnessed by attender.
- Weakness resolved on arrival to the hospital; now complain of a headache.
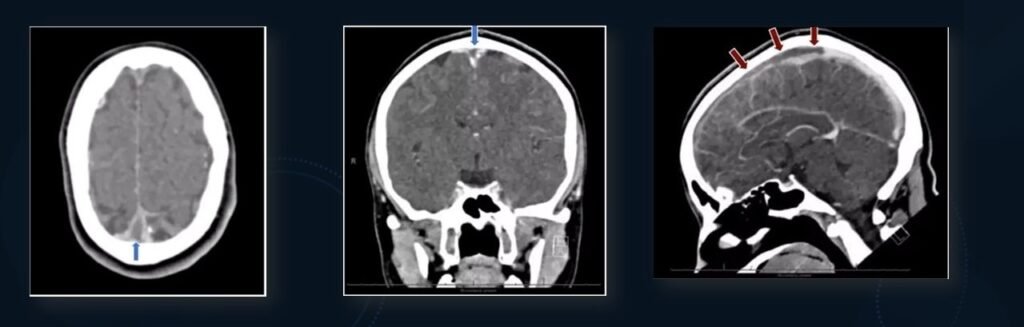
FILLING DEFECT OF SUPERIOR SAGITTAL SINUS, EXTENDING BILATERALLY INTO THE TRANSVERSE SINUSES AND VEINS OF TROLLARD. EMPTY DELTA SIGN IS SEEN.
Neurological Exam:
- Alert.
- No cranial nerve deficits.
- Normal and equal strength bilaterally.
- Intact sensation in all dermatomes.
- Normal cerebellar testing.
- Normal gait.
- Non-contrast head CT was done.
BRAIN MRI: SUBTLE LOSS OF THE FLOW VOID INVOLVING THE HIGH SUPERIOR SAGITTAL SINUS,WHICH MAY REFLECT A SMALL AMOUNT OF THROMBOSIS EXTENDING INTO THE SUPERIOR SAGITTAL SINUS

MR VENOGRAM: A THROMBOSED CORTICAL VEIN OVERLYING THE LEFT FRONTAL AND PARIETAL LOBES AND EXTENDING ALONG THE LEFT LATERAL PARIETAL CONVEXITY. NO FLOW RELATED SIGNAL IS IDENTIFIED IN THIS VESSEL
IMPRESSION:
- Thrombosed cortical vein overlying the high left frontal parietal convexity with findings concerning for venous ischemia involving the left posterior frontal parietal lobes.
- A small component of thrombosis may extend into the superior sagittal sinus.
- Additionally, a punctate focus of adjacent susceptibility artifact is noted involving the left parietal lobe, possibly reflecting petechial haemorrhage.
DIAGNOSIS:
CEREBRAL VENOUS SINUS THROMBOSIS
- YOUNG PATIENT
- ON HARMONAL BIRTH CONTROL PATCH
- CT SHOWS MIDLINE HYPERDENSITY CORRESPONDING TO LOCATION OF SUPERIOR SAGITTAL SINUS.
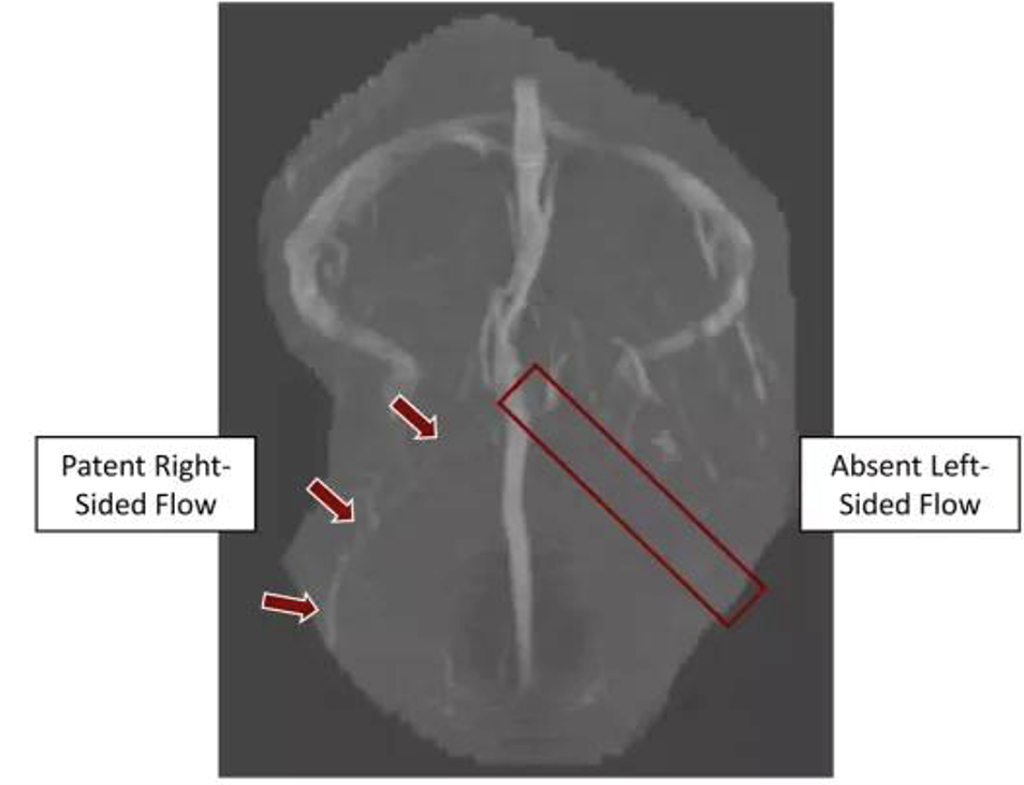
- CT VENOGRAM WAS ORDERED.
CT VENOGRAM: