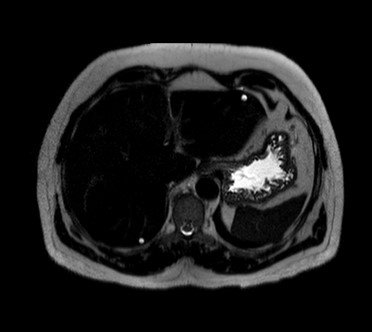
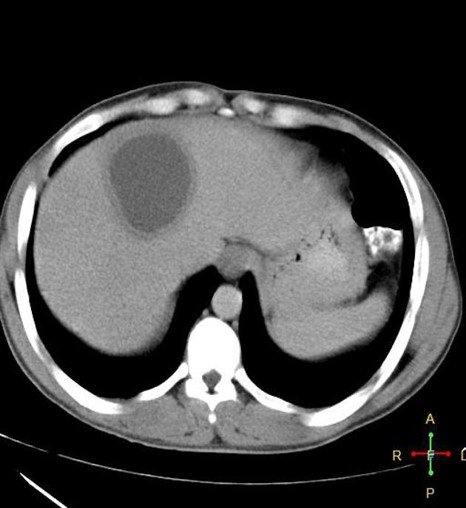
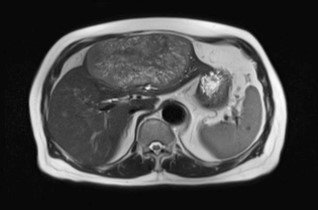
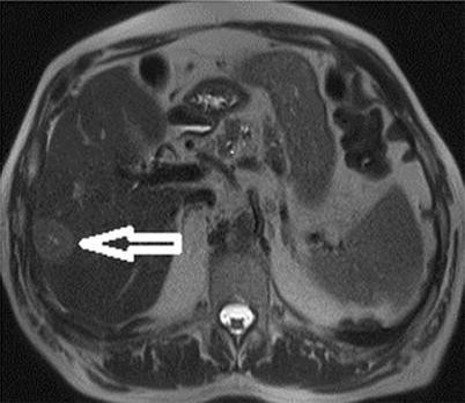
T2: Two rounded lesions following fluid signal seen at segment 2 and 6 of the liver.
Focal Nodular Hyperplasia (FNH)
–Hyperplastic lesion, common in young females
–Intense homogeneous arterial enhancement
–Central scar characteristic
–Scar enhances on delayed phase
–MRI: T2 hyperintense scar
–No malignant potential
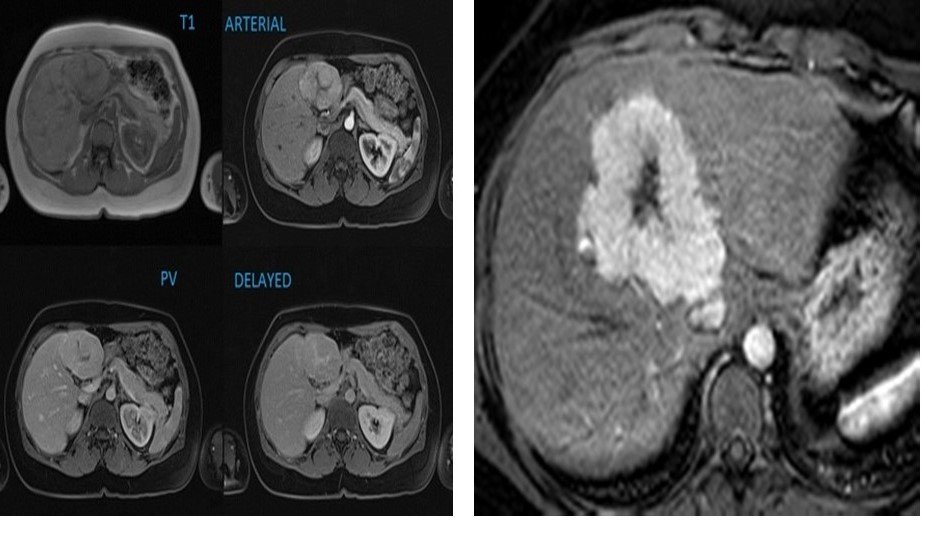
Summary of T1, and the various phases of the contrast study illustrating the nature of the focal liver lesion.
Note the enhancement of the central scar only on the delayed images when the rest of the lesion has washed out.
On the arterial phase, the lesion demonstrates intense homogenous enhancement, except for the central scar.
Hepatic Adenoma
–Benign neoplasm associated with OCPs/steroids
–Hypervascular arterial enhancement
–No central scar
–MRI shows fat with signal drop on out-of-phase
–Risk of hemorrhage
–Small risk of malignant transformation
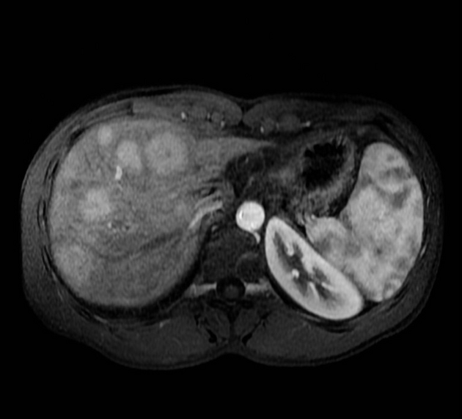
The largest lesion is located in the left lobe of the liver, segment 3, and demonstrates isointense signal compared to liver on T1 weighted images and no signal drop out on out-of-phase imaging to suggest presence of fat.
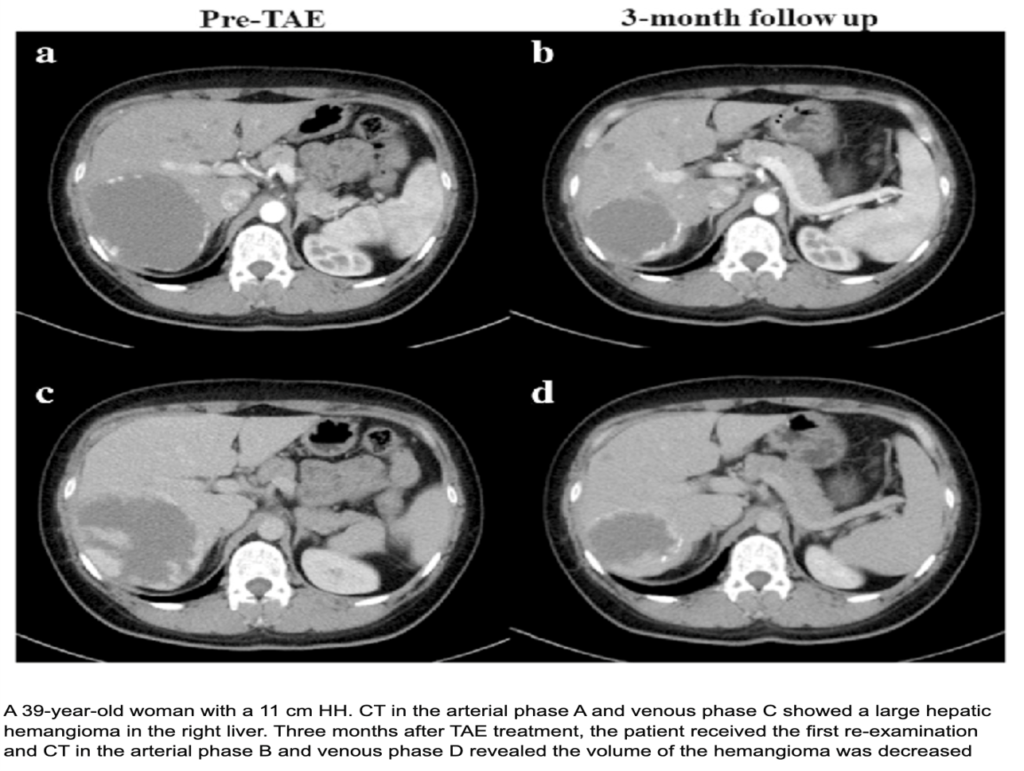
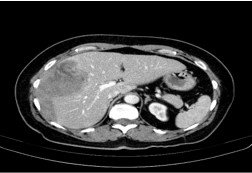
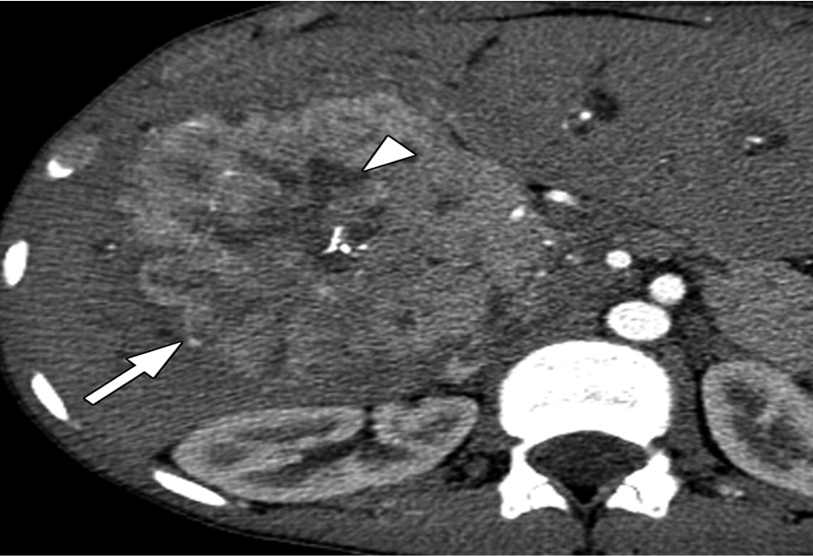
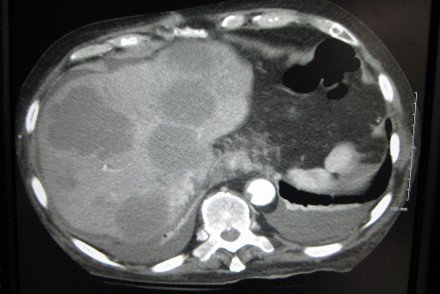
Heterogeneous mass measuring 13.3 x 11.1 x 9.7 cm, seen involving segment VIII and segment V in the right hepatic lobe, with hyperdense subsapsular hematoma at corresponding lateral hepatic surface and free intra-peritoneal hemorrhage.
Amoebic Liver Abscess
–Most common liver abscess in India
–Usually solitary, right lobe
–Hypodense lesion with peripheral rim enhancement
–No internal septations
–Clinical fever and RUQ pain
–Anchovy sauce aspirate
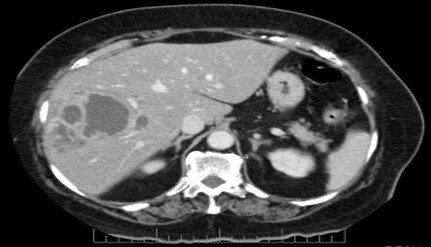
Solitary cystic liver lesion with low attenuation center and peripheral thick enhancing wall.
CT Findings are consistent with amebic liver abscess.
Solitary cystic liver lesion with low attenuation center and peripheral thick enhancing wall.
CT Findings are consistent with amebic liver abscess.
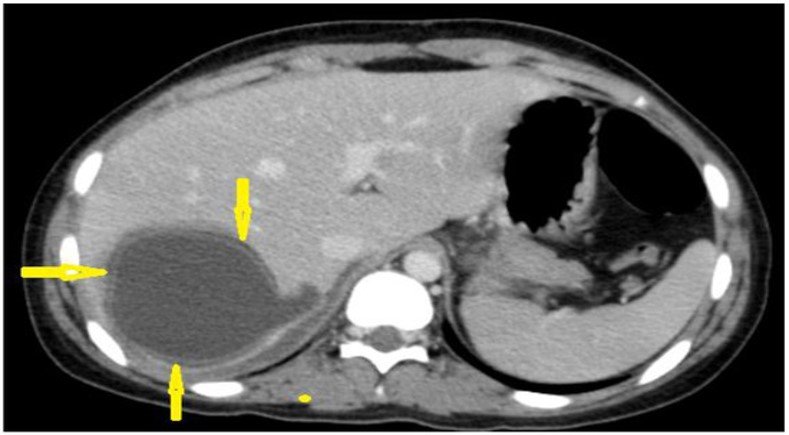
Contrast-enhanced computed tomography of a 15-year-old female presenting with abdominal pain showing a well-circumscribed, unilocular, non-enhanced cystic lesion in the right lobe of the liver with typical “double-wall sign” of hydatid cyst (arrows).
Cyst in the liver with daughter cyst.
Tubercular Liver Abscess
–Rare, usually immunocompromised
–Multiple small hypodense lesions
–Minimal peripheral enhancement
–Often associated with TB elsewhere
–Diagnosis by biopsy
–Responds to ATT
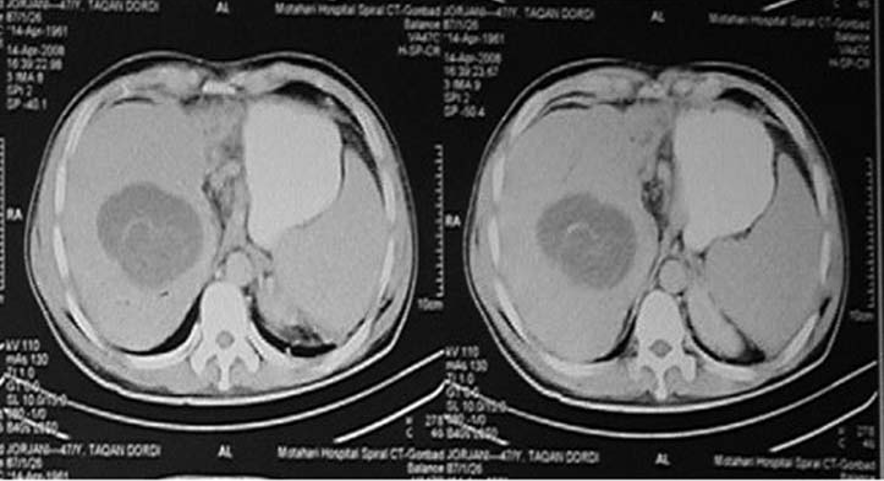
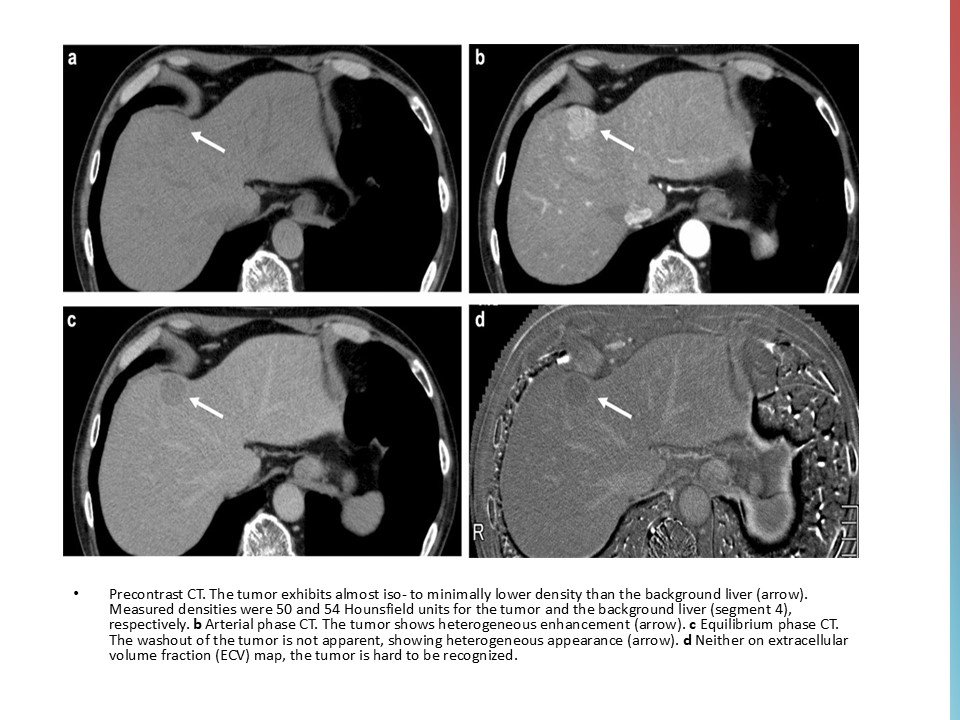
CT and MR images in a 37-year-old male with poorly-differentiated HCC with histological capsule. METAVIR score of the background liver was F3. In contrast-enhanced CT, a 49-mm observation shows (a) nonrim APHE on arterial phase and (b) nonperipheral washout with an enhancing capsule on equilibrium phase. In gadoxetic acid-enhanced MRI, a 48-mm observation shows (c) nonrim APHE on arterial phase, (d) nonperipheral washout on portal venous phase, and (e) TP hypointensity with suspicion of an enhancing capsule on transitional phase. Hepatobiliary phase image clearly shows (f) a nonenhancing capsule surrounding the observation.
Cholangiocarcinoma
–Malignancy of bile duct epithelium
–Hypodense lesion on NCCT
–Progressive delayed enhancement
–Capsular retraction common
–Biliary dilatation present
–Poor prognosis
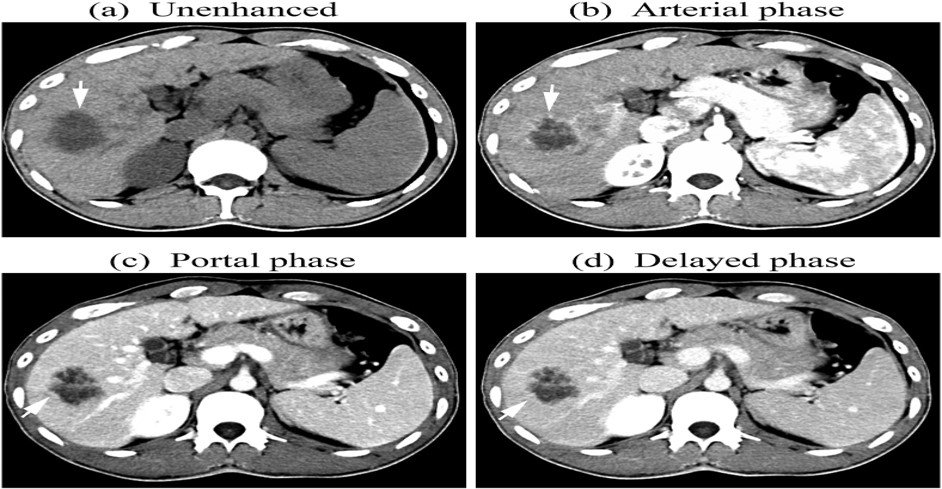
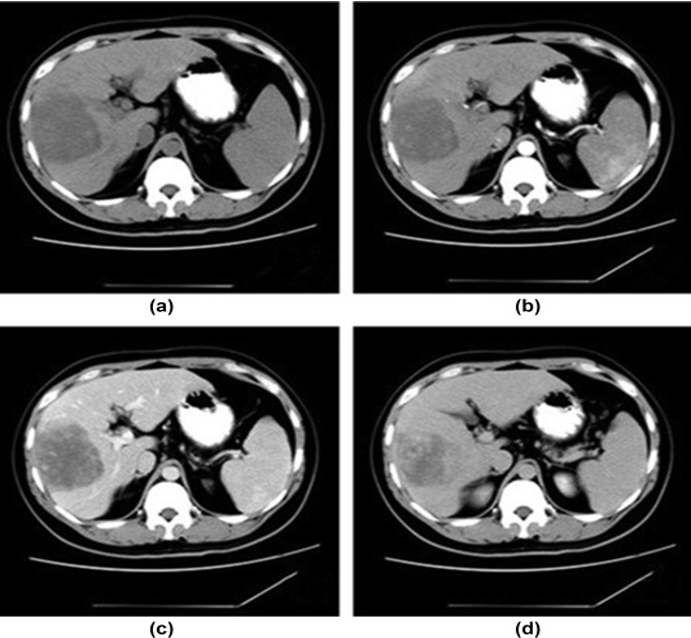
(a) unenhanced, (b) Arterial, (c) portal, and (d) delayed phases. After intravenous contrast administration, the nodule shows stable peripheral rim-like enhancement (arrow).
Fibrolamellar HCC
–Variant of HCC in young adults
–Occurs in non-cirrhotic liver
–Large solitary mass
–Central scar present
–AFP usually normal
–Better prognosis than classic HCC
T2 :Hypo to slightly hyperintense
Central scar
Angiosarcoma
–Rare aggressive malignant tumor
–Multiple hemorrhagic lesions
–Heterogeneous enhancement
–Associated with vinyl chloride/arsenic
–Rapid progression
–Very poor prognosis
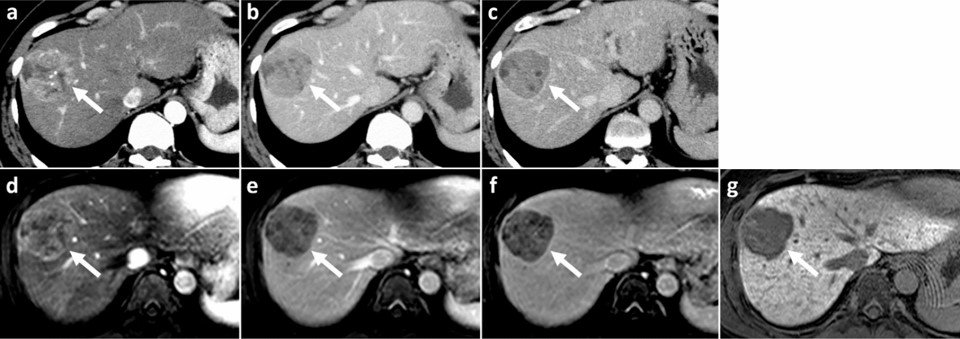
A 33-year-old male patient with right hepatic haemangiosarcoma. (a) Unenhanced CT image shows a lobulate mass with an indistinct boundary in the right lobe. (b–d) Enhanced CT images of the arterial, venous, and delay phases showed a heterogeneous centripetal enhancement of the mass, and the contrast agent did not completely fill in the lesion at the end.
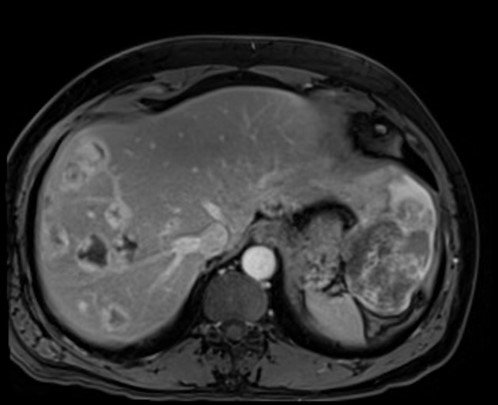
T1 C+ (Gd)
heterogeneous enhancement with progressive filling
irregular flame-shaped pattern
Colorectal Cancer Metastases
–Most common source of liver metastases
–Multiple hypodense lesions
–Peripheral rim enhancement
–Hypovascular metastases
–Often asymptomatic initially
Target appearance
Axial CT of the abdomen showing multiple liver metastases.
Breast Cancer Metastases
–Multiple variable-sized lesions
–Hypodense on CT
–Delayed enhancement pattern
–Capsular involvement common
–Associated bone metastases
–Advanced disease marker
Target appearance
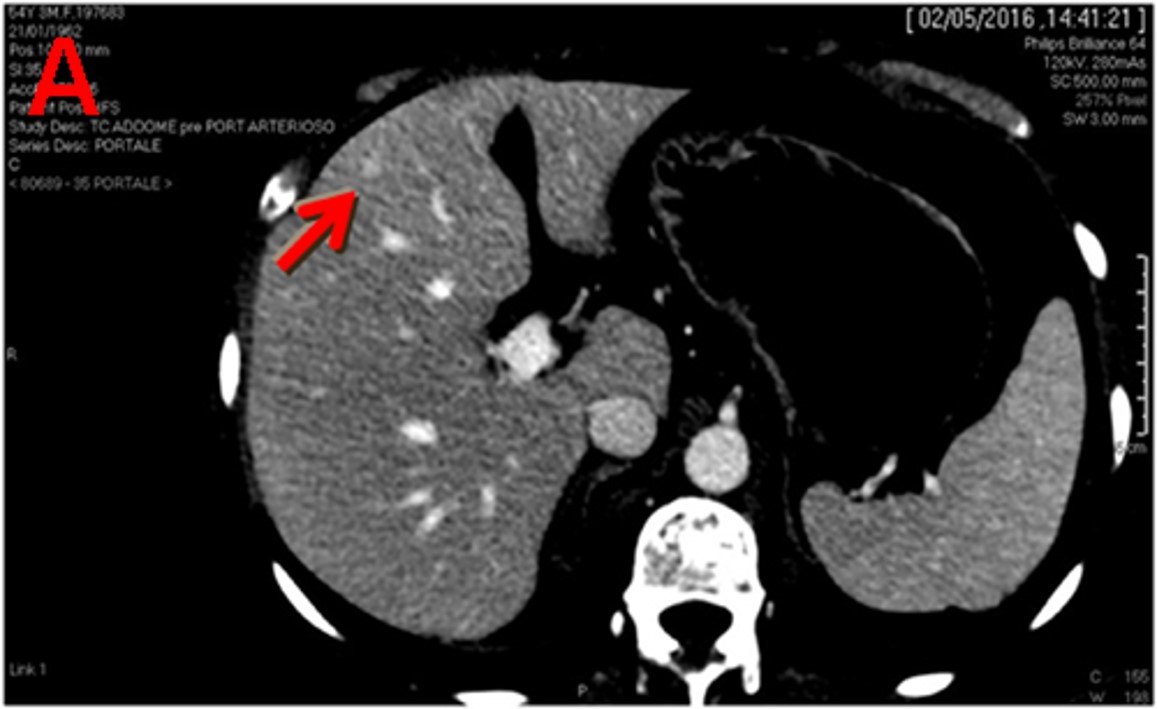
Computed tomography (CT) scan performed in April 2016 shows three liver lesions (LLs) in arterial phase. a. The arrow indicates LL (diameter: 7 mm) with contrast enhancement suspected of metastasis at 4th segment.